Case history:
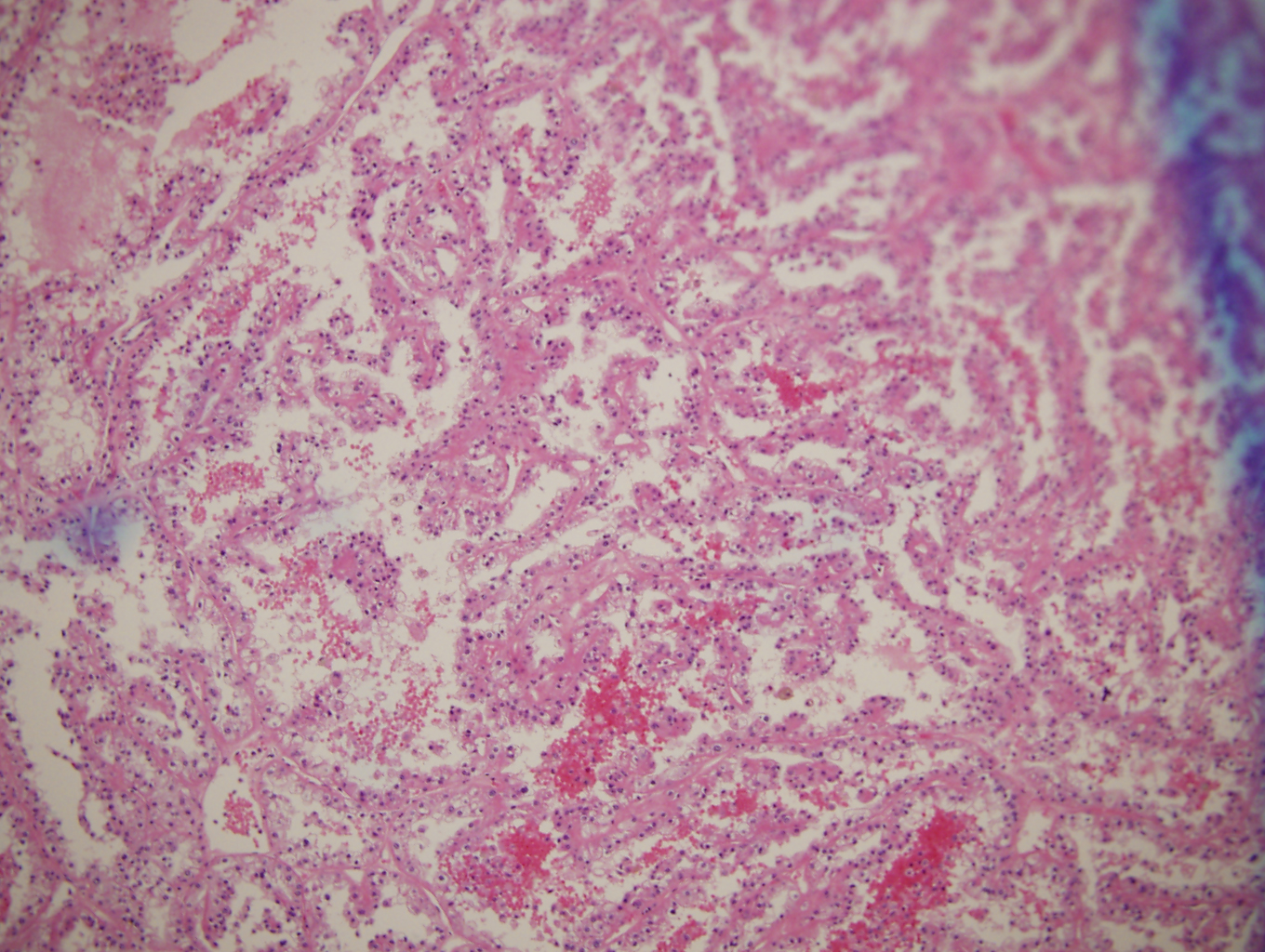
The patient is a 64 year-old female with clinical history of relapsing/remitting multiple myeloma. CBC data: WBC 5.9 cells/microliter with a differential of 70% segs, 20.5% lymphs, 8.5% monos, 0.3% eos and 0.2% basos. PLT 144,000 /microliter, MCV 99 fL, Hemoglobin 8.9 gram/deciliter and HCT 28%. A surveillance bone marrow performed at OSH and showed increase of plasma cells and additional finding on the biopsy as illustrated.Diagnosis:
A. Protein (Ig) deposits
B. Amyloid
C. Platelet clumps
D. Marrow necrosis
The answer is “C. Platelet clumps”
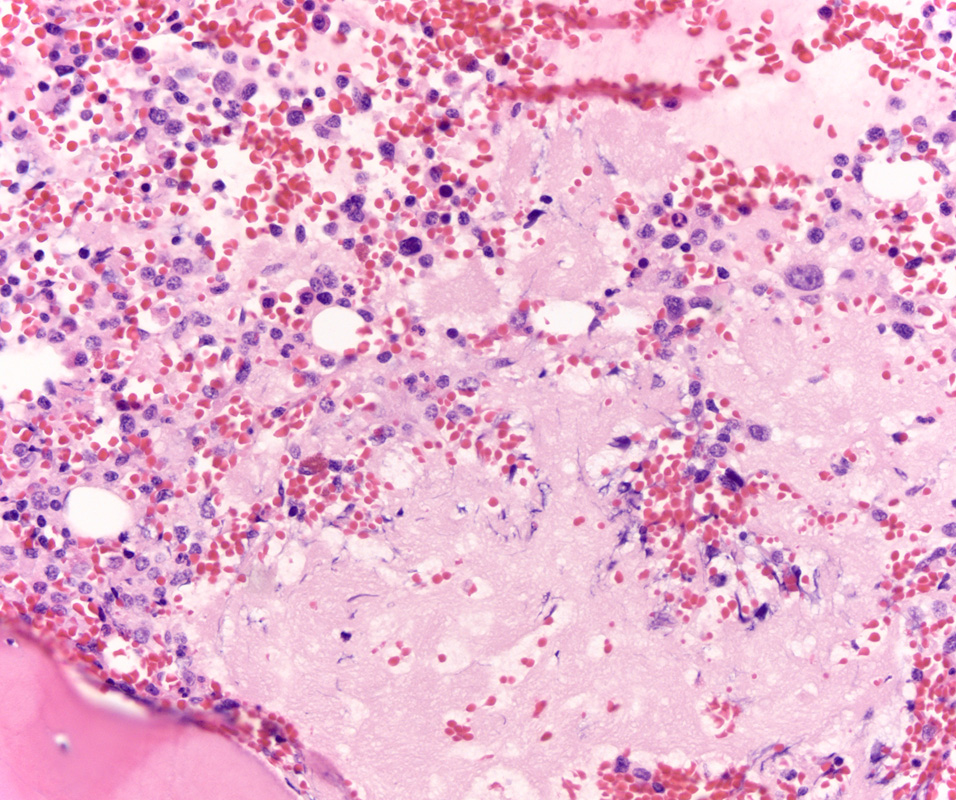
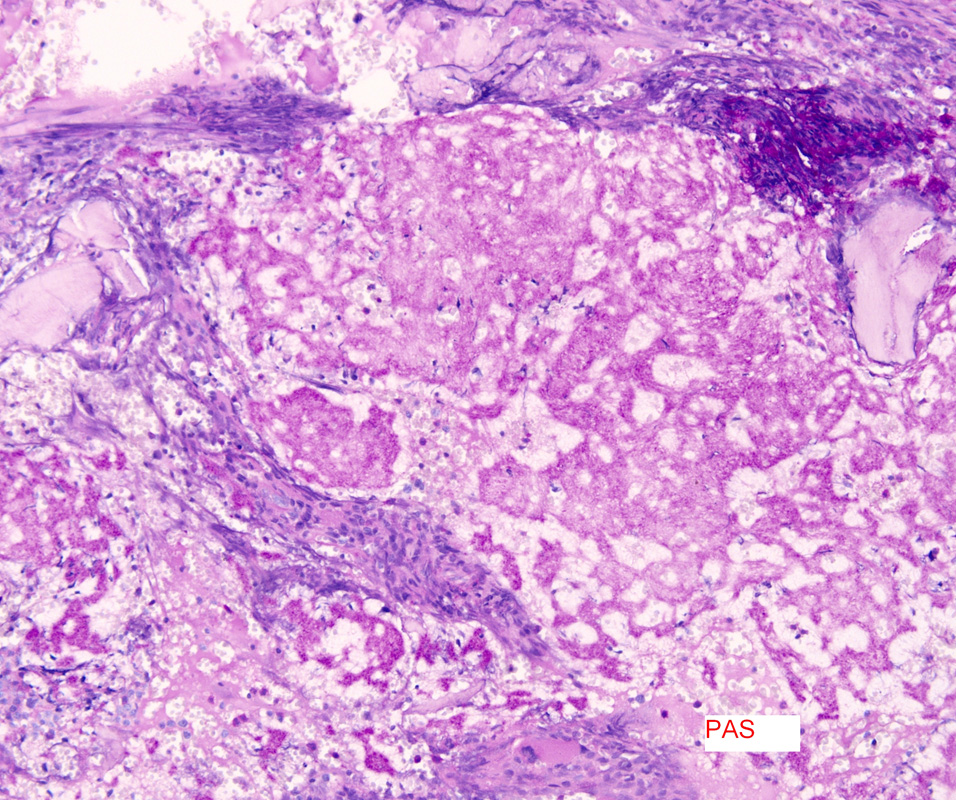
Higher magnification and PAS stain show fluffy “cotton candy” like material next to plasma cell infiltrates compatible with platelet clumping/fibrin material. Congo red stain was negative; in addition, examination under Texas red filtration was negative for amyloid. Congo red evaluation under Texas red filtration (red-fluorescence) is superior in identifying amyloid deposits, and more reliable than polarized light alone. Other considerations such a marrow necrosis and protein deposits excluded based on the PAS staining. Platelet clumping/fibrin clots are not uncommon on bone marrow trephine biopsies.
Ref: Clement CG et al. An evaluation of Congo red fluorescence for the diagnosis of amyloidosis. Human Pathology. 2014. Aug;45(8):1766-72.
Case contributed by Vishnu Reddy, M.D., Professor, and Interim Division Director, Anatomic Pathology, Neuropathology, UAB Department of Pathology