Case history:
Teenager with thyroid mass.
Diagnosis:
- Poorly differentiated thyroid carcinoma
- Alveolar rhabdomyosarcoma
- Adamantinoma-like Ewing sarcoma
- NUT carcinoma
Answer:
“C” Adamantinoma-like Ewing sarcoma
Discussion:
This case showed the following immunophenotype:
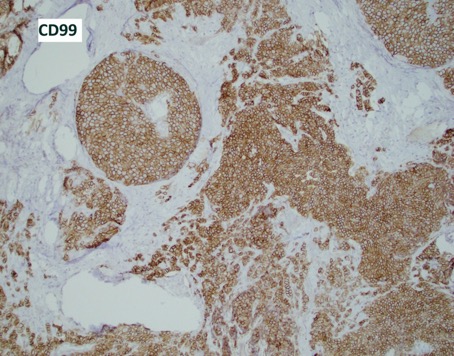
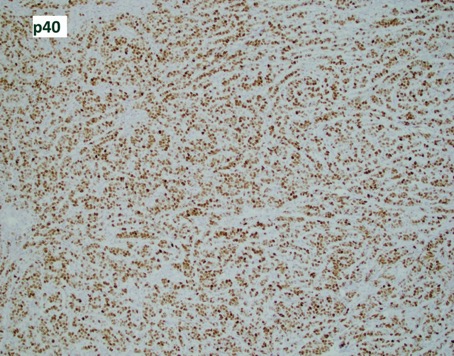
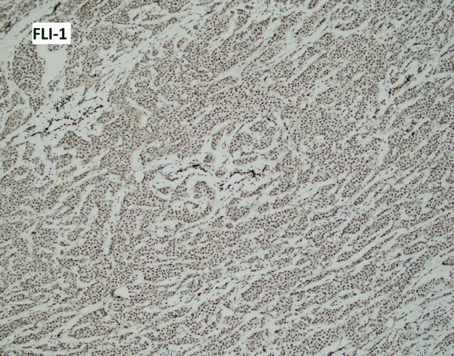
Positive: Pankeratin (diffuse), CD99 (diffuse, strong and membranous), FLI-1 (nuclear), p40 (diffuse, nuclear), rare positive cells for synaptophysin.
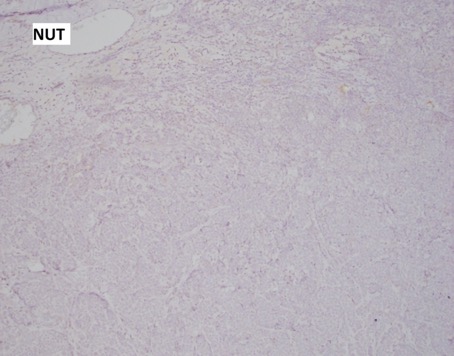
Negative: Thyroglobulin, TTF1, PAX8, Calcitonin, CK20, SOX10, ERG, SMA, NUT.
An EWSR1-FLI1 fusion was identified by RT-PCR.
Diagnosis: Ewing sarcoma with epithelial differentiation (adamantinoma-like Ewing sarcoma).
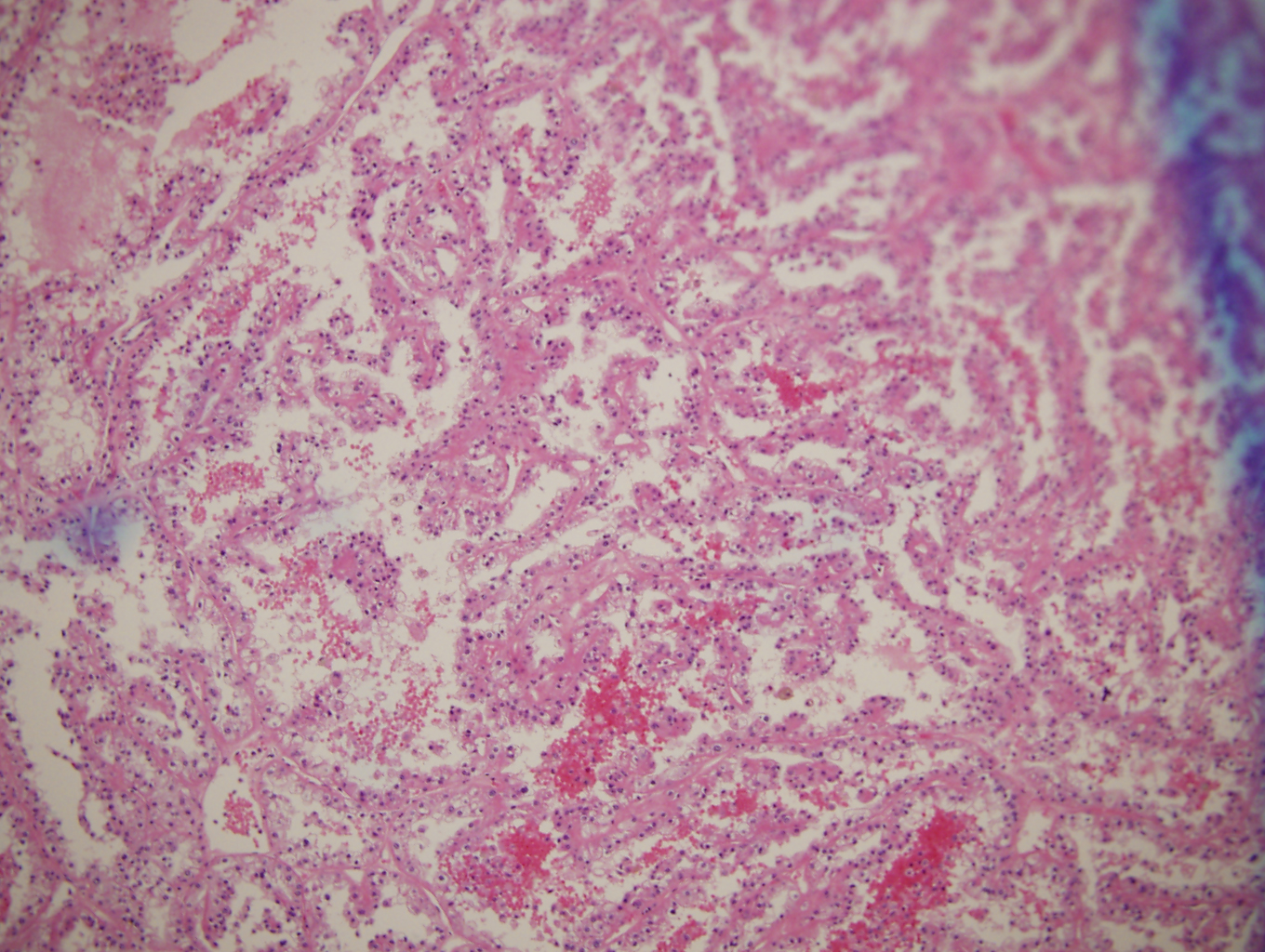
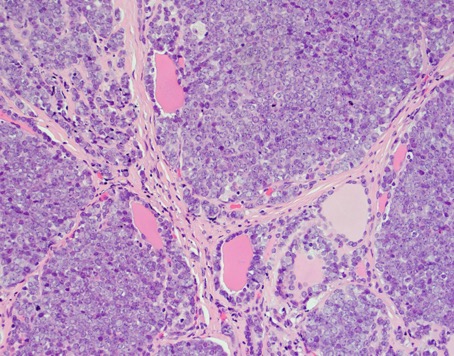
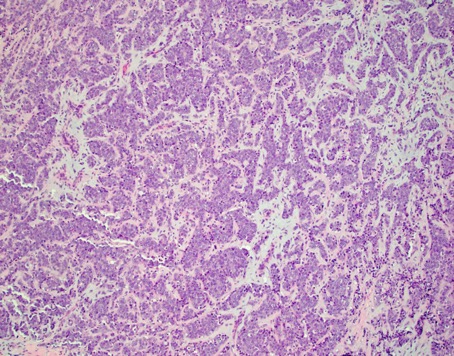
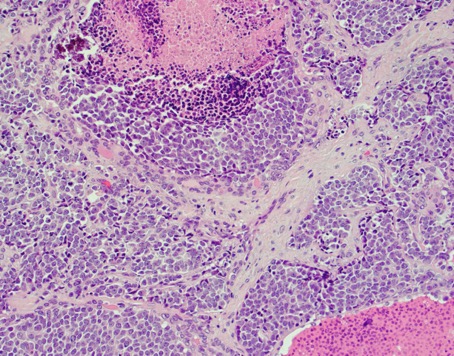
Ewing sarcoma (ES) family of tumors are defined by recurrent translocations involving EWSR1 and an ETS gene, namely FLI1 or ERG. Classic Ewing sarcoma histologically features monotonous small to medium sized blue cells growing in lobules and sheets with variable pseudorosette formation. Nuclei show vesicular chromatin and the cytoplasm is scant and clear. While not specific, membranous immunoreactivity for CD99 is typical. In about 20-30% of ES cases, cytokeratin expression can be found, usually focal. However, some ES can show complex epithelial differentiation at the light microscopic level (squamous pearls and bridges) as well as diffuse expression of cytokeratins, p40, and high molecular weight keratins. These so called “adamantinoma-like Ewing sarcomas” occur in bone and in head and neck sites such as parotid, sinonasal tract, thyroid, etc.
While admittedly adamantinoma-like Ewing sarcomas do not resemble adamantinomas of bone, this is a historical name that exists because the first such cases of adamantinoma-like Ewing sarcoma were described in long bone.
Depending on the site involved in the head and neck, adamantinoma-like Ewing sarcoma has varied differential diagnosis. NUT carcinoma, myoepithelial carcinoma, and synovial sarcoma should be excluded in all sites. In the parotid, basal cell adenocarcinoma is a differential consideration. In the sinonasal tract, sinonasal undifferentiated carcinoma and olfactory neuroblastoma are mimics. In the thyroid, SETTLE and poorly differentiated thyroid carcinoma should be excluded. Molecular confirmation is necessary to make a definitive diagnosis of adamantinoma-like Ewing sarcoma. So far, all cases have shown an EWSR1-FLI1 fusion. Accurate diagnosis of adamantinoma-like Ewing sarcoma is critical to ensure the patient receives the proper chemotherapy protocols.
Reference: Bishop JA, et al. Adamantinoma-like Ewing Family Tumors of the Head and Neck: A pitfall in the differential diagnosis of basaloid and myoepithelial carcinomas. AJSP. 2015; 39 (9): 1267-1274.
Case contributed by Todd Stevens, M.D., Assistant Professor, Anatomic Pathology, UAB Department of Pathology