Case History
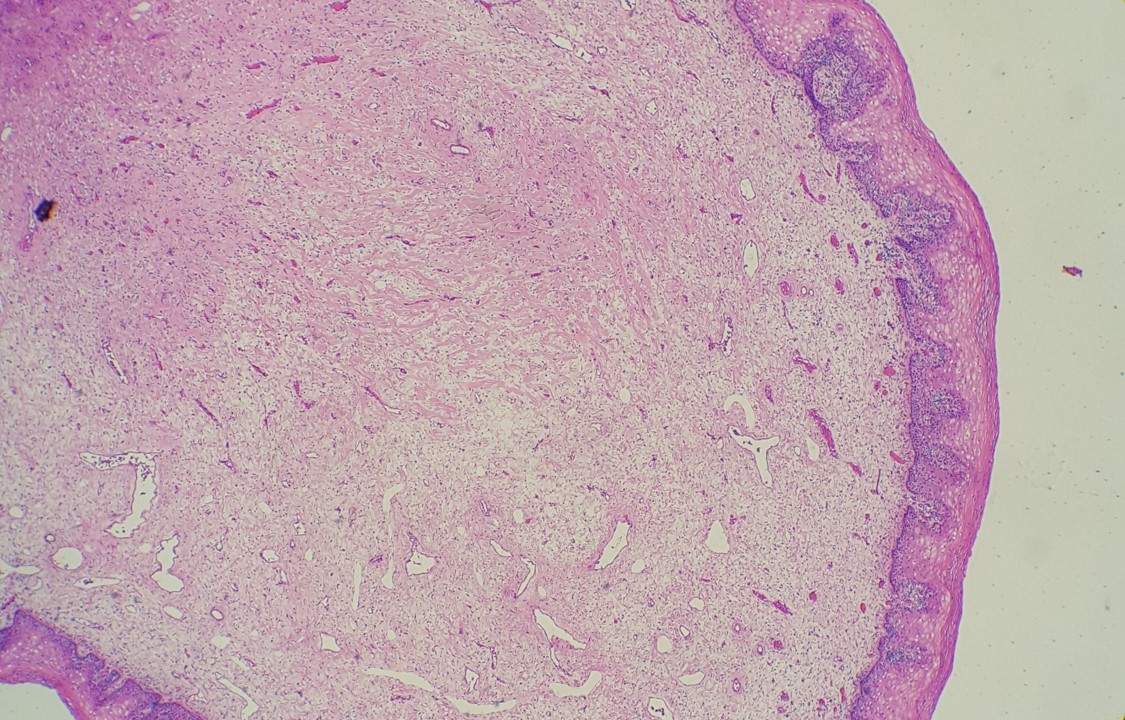
45-year-old female presents with a ruptured hemorrhagic ovarian mass. The mass was received in fragments and measures 7.5 x 5.7 x 4.3 cm in aggregate. Grossly unremarkable fallopian tube is also present. IHC staining for inhibin revealed positive staining in the cells of interest & EMA was negative.
What is the diagnosis?
- Endometrioid adenocarcinoma, FIGO 3
- High grade serous carcinoma
- Low grade serous carcinoma
- Granulosa cell tumor, adult type
Answer: D. Granulosa cell tumor, adult type.
Explanation:
These tumors account for approximately 10% of sex cord stromal tumors and about 2 to 3% of all primary ovarian cancers. These are low-grade malignant tumors that typically present as an adnexal mass in a peri-or postmenopausal woman. These tumors can be associated with estrogenic manifestations such as disordered proliferative endometrium or endometrial hyperplasia and even endometrioid adenocarcinomas. A small percentage of cases present as a result of tumor rupture and hemoperitoneum.
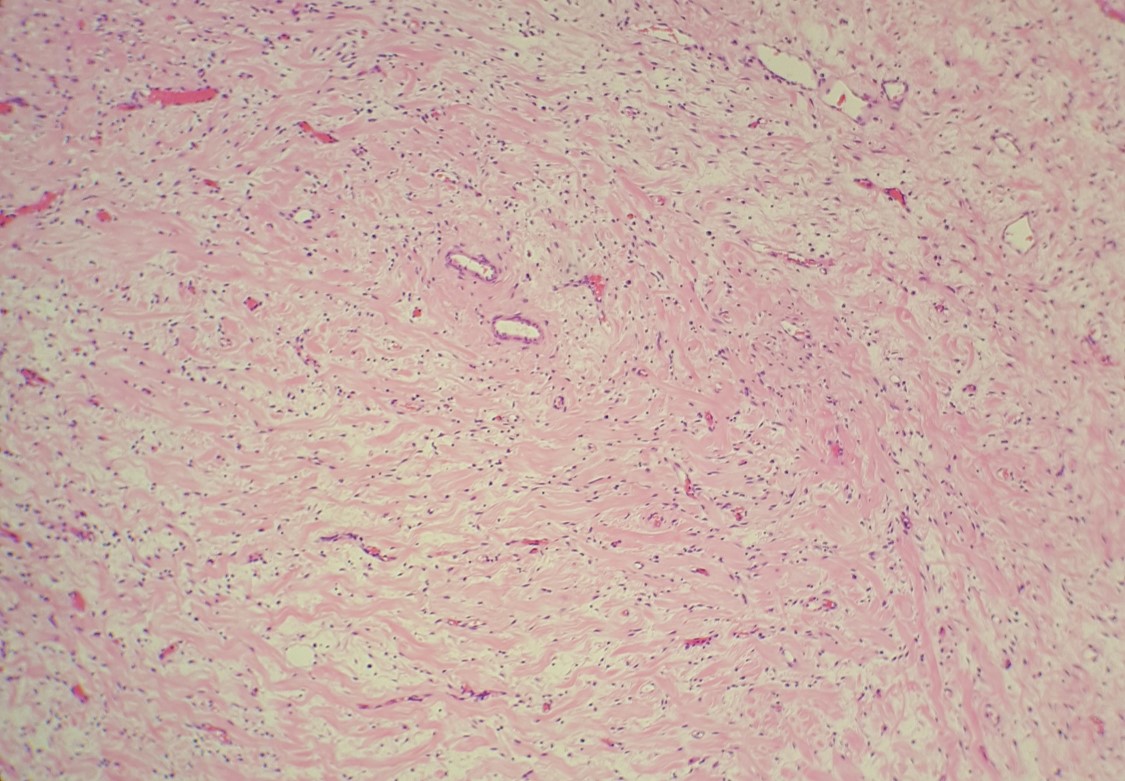
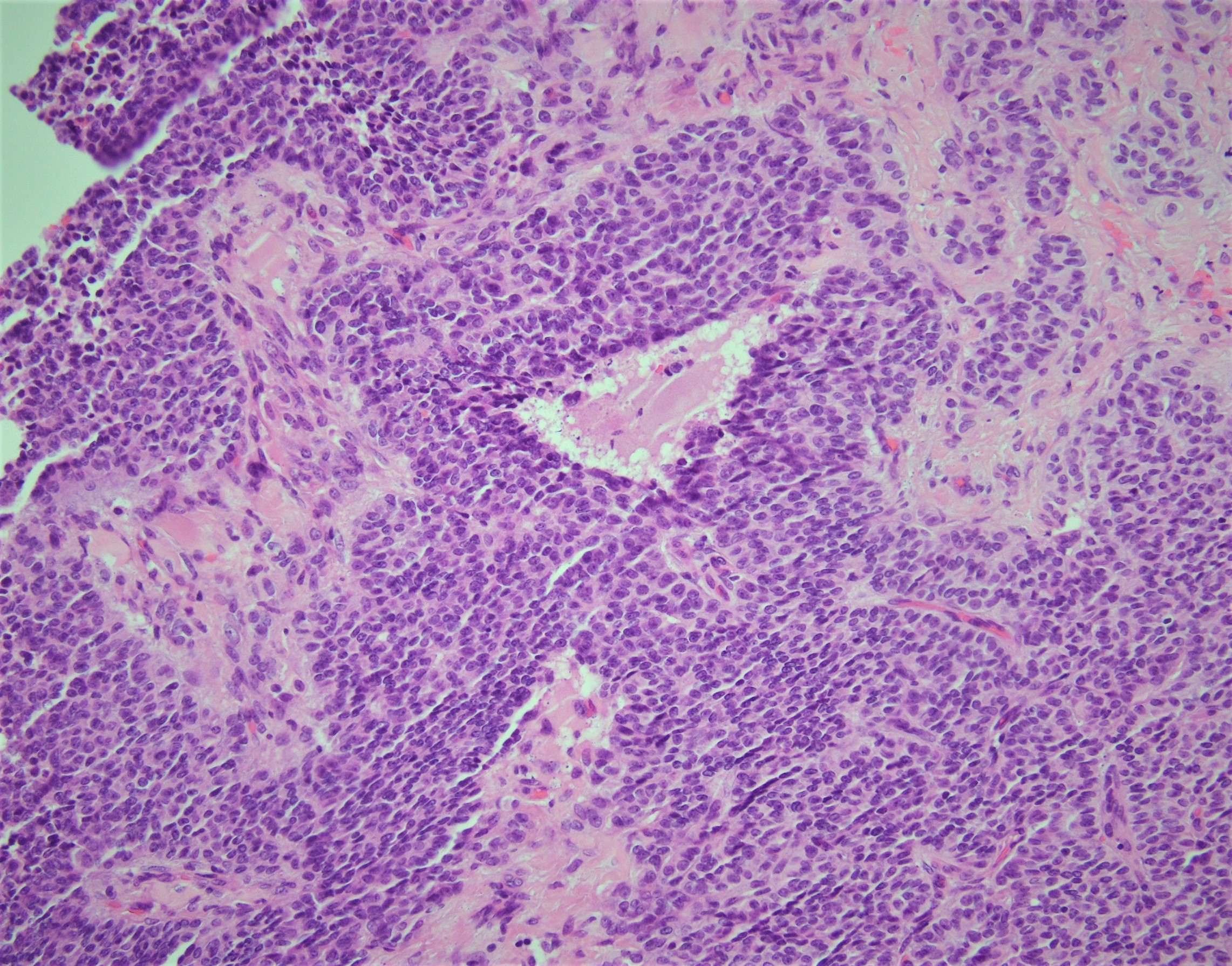
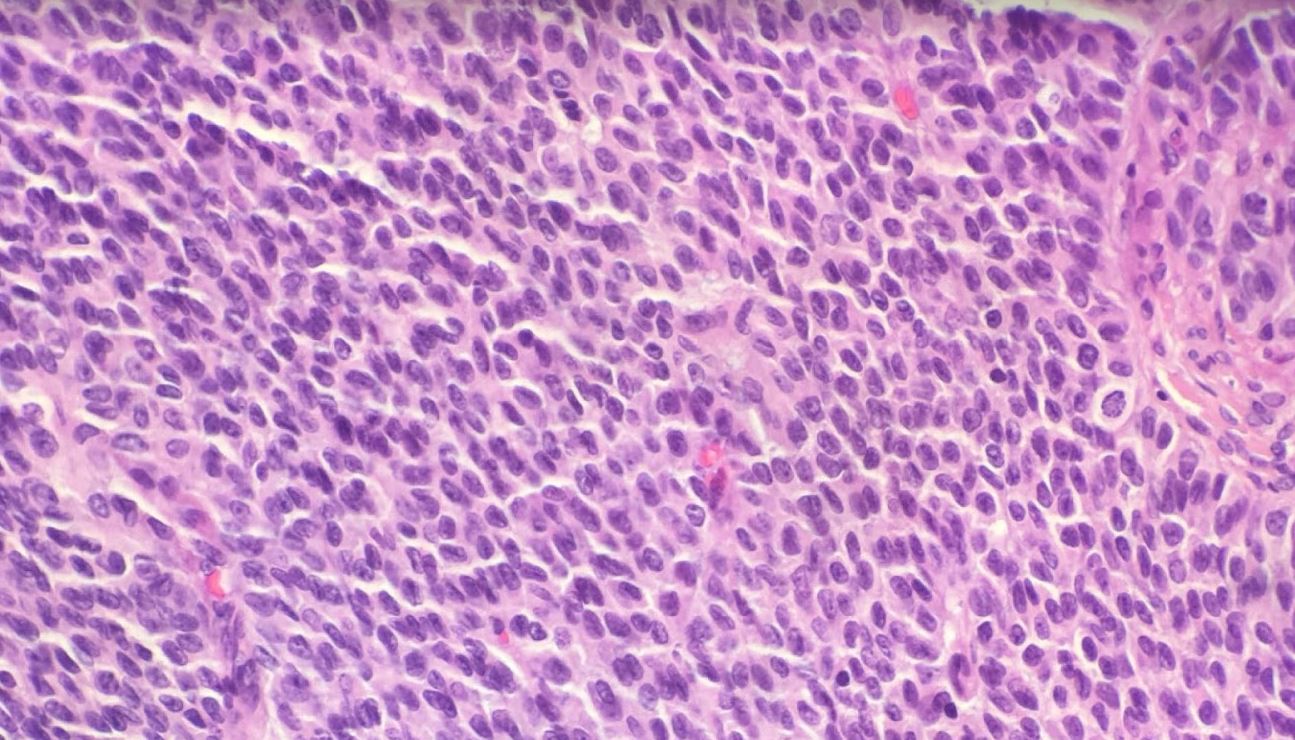
Histologically, the neoplastic cells comprising these neoplasms show scant cytoplasm and oval to angulated nuclei with prominent nuclear grooves such as in this case. Architecturally, these neoplasms can present in a wide variety of histologic patterns.
AGCTs are typically reactive for inhibin and calretinin and are negative for EMA. Additionally, these neoplasms were shown to have a single-point mutation in the FOXL2 gene.
Case contributed by: Dina Kokh, M.D., Assistant Professor, Anatomic Pathology