Case History
A 35-year-old female with multiple cutaneous lesions that show these histopathologic features. This patient should be screened for a germline mutation of which gene and will likely develop which types of tumors in addition to the one displayed here?
- BHD, renal cell carcinoma, fibrofolliculoma, trichodiscoma
- PTCH1, basal cell carcinomas, medulloblastoma
- SDHB, pheochromocytomas, paragangliomas
- FH, renal cell carcinoma, uterine leiomyomas
Answer:
D.) FH, Renal Cell Carcinoma, multiple cutaneous and uterine leiomyomas __ (Example “A”, Granular cell tumor)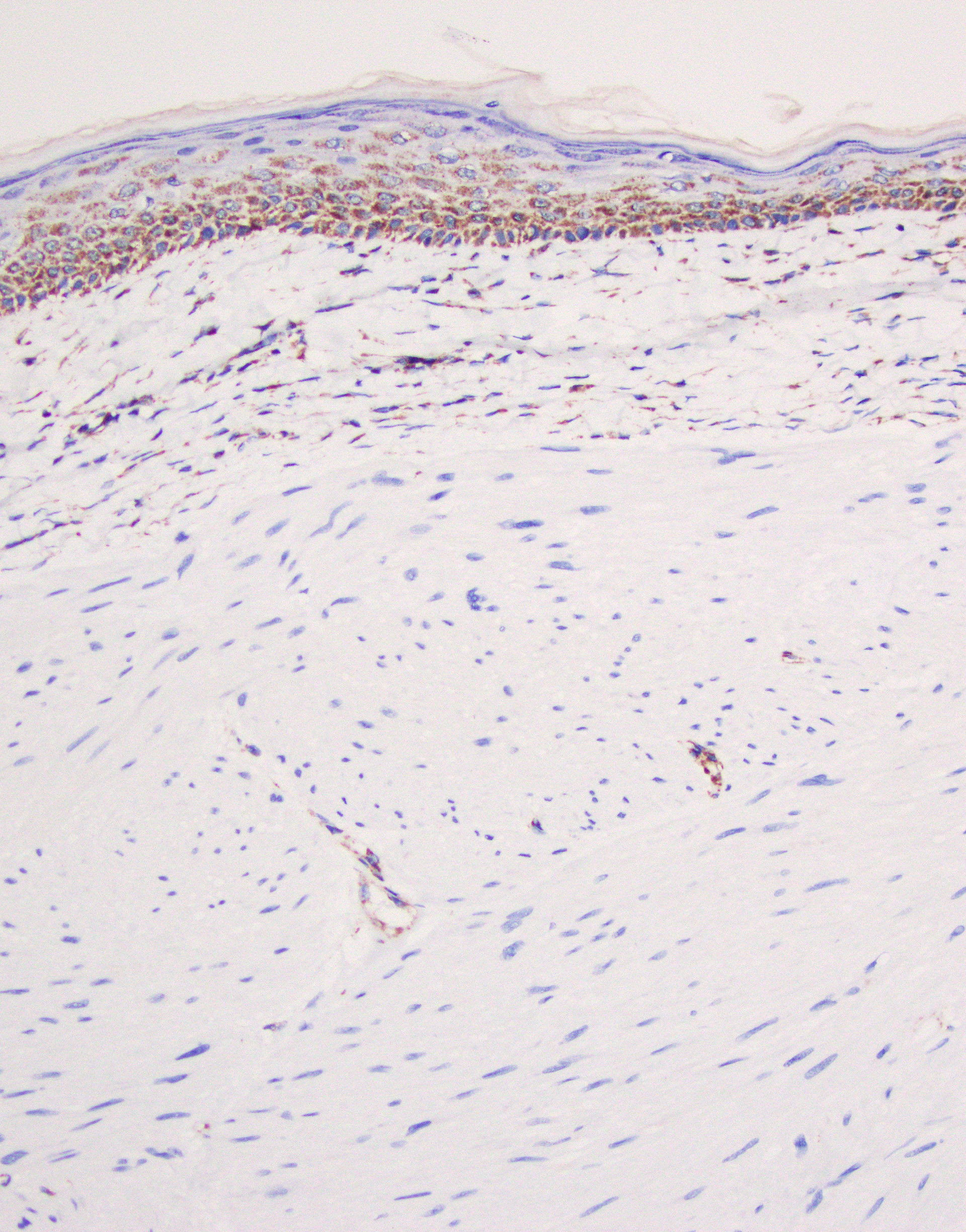
A brief explanation of the answer and summary of the histomorpholgoic findings, immunohistochemistry, clinical presentation, and other pertinent information needed to make the diagnosis.
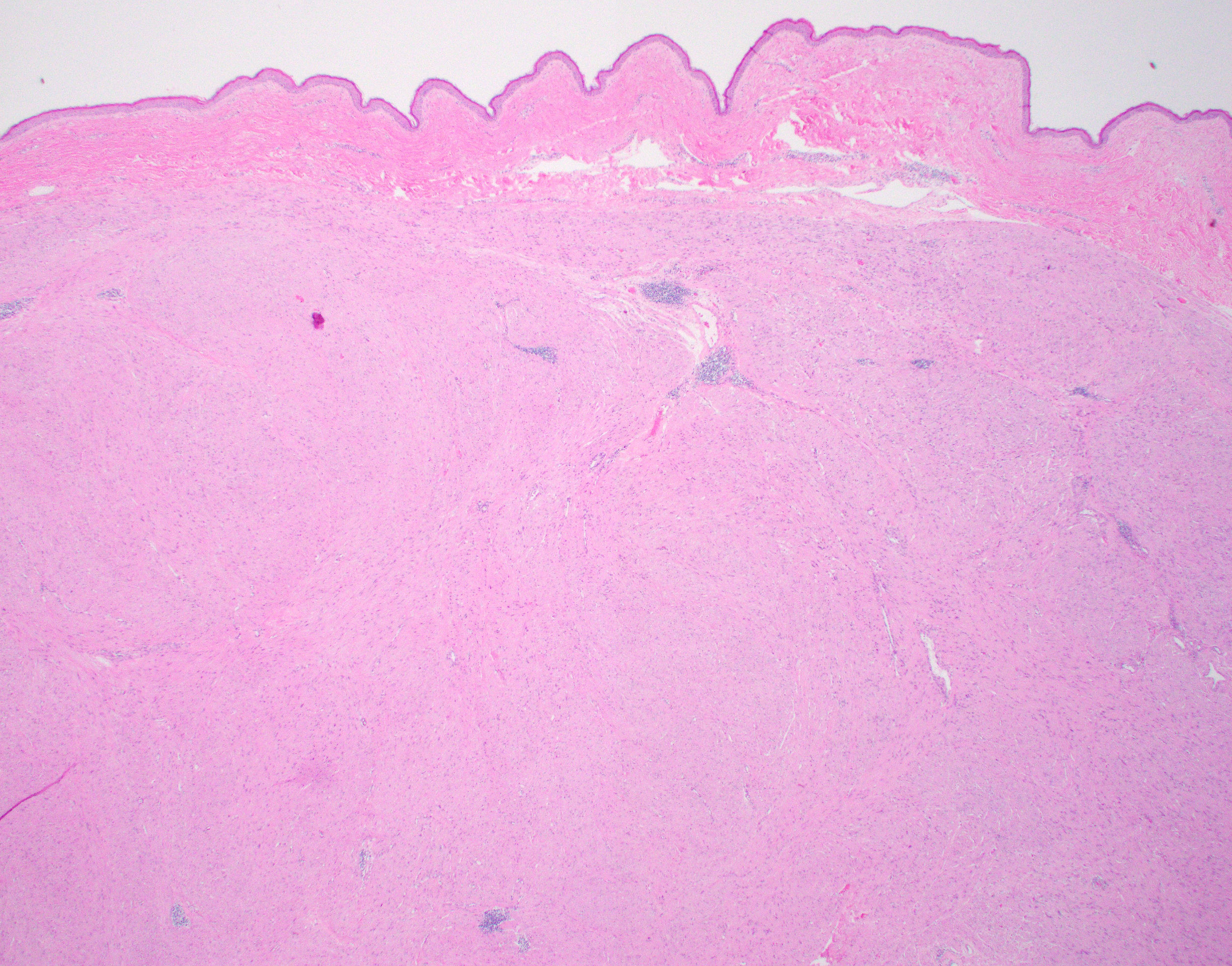
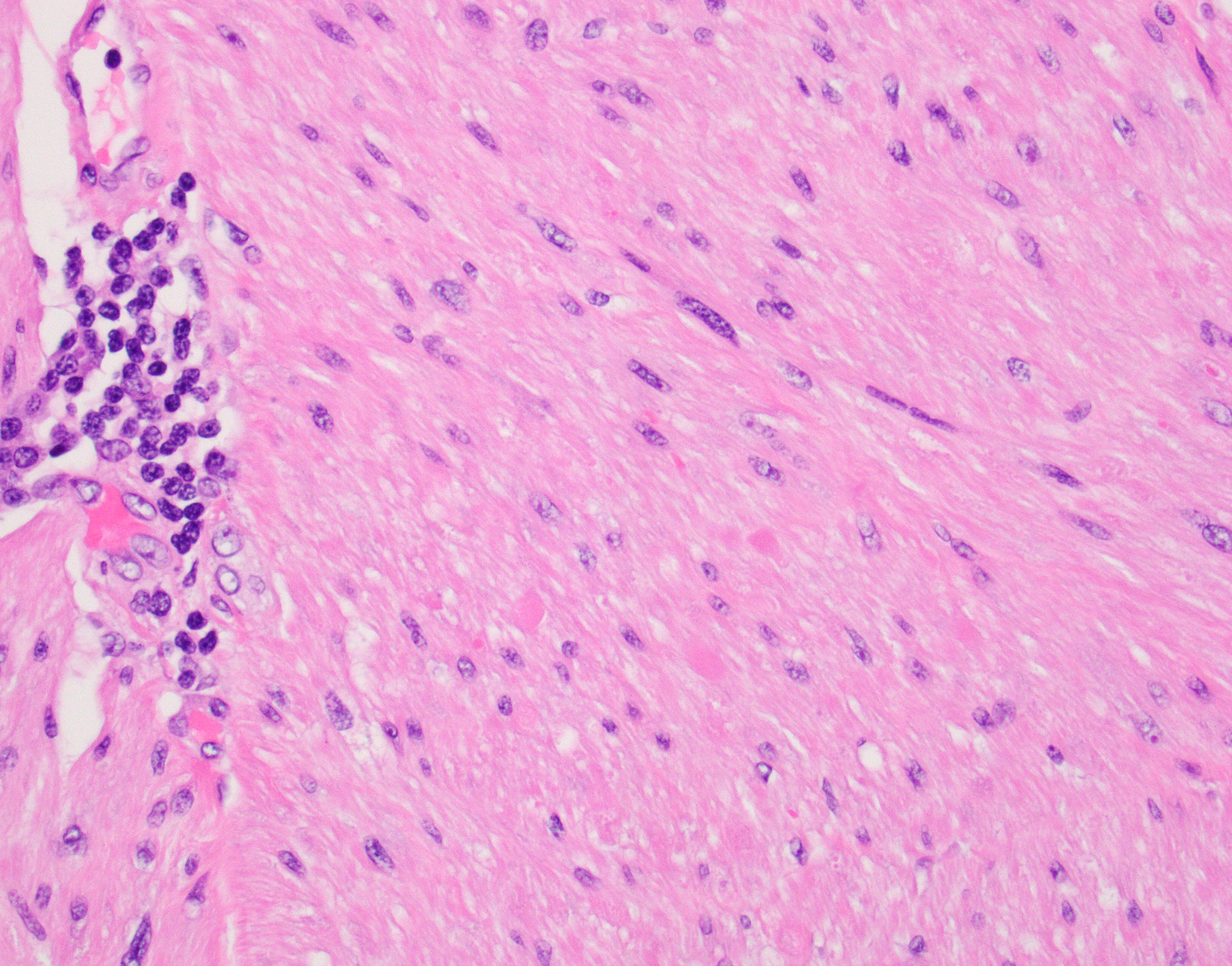
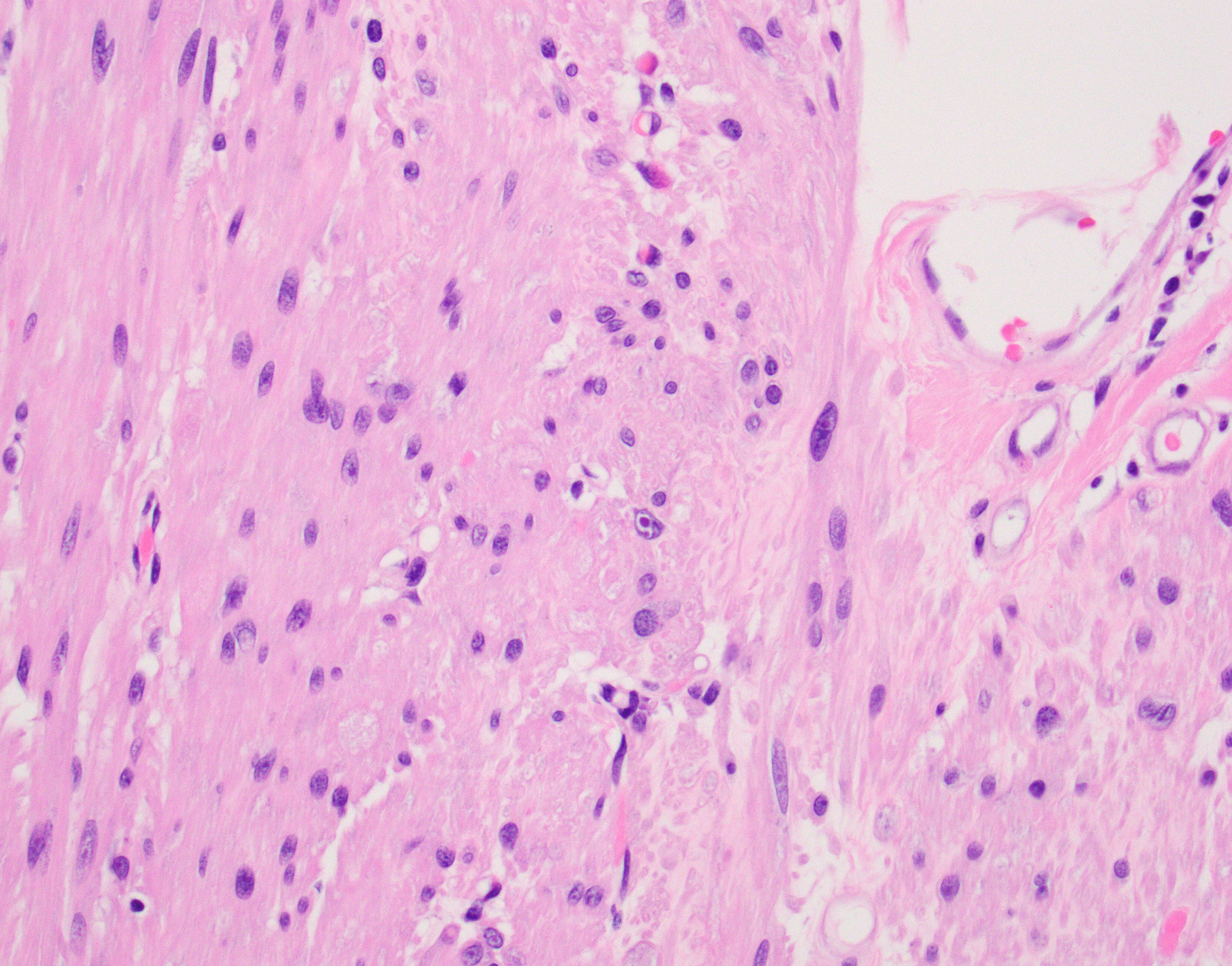
The patient is showing well-circumscribed (Fig 1) leiomyomatous lesions with features of the Hereditary Leiomyomatosis and Renal Cell Cancer (HLRCC) Syndrome (OMIM 150800, AKA Reed’s syndrome) which is produced due to germline mutations of the gene coding for the mitochondrial enzyme Fumarate Hydratase (FH, 1q43). This syndrome is characterized by multiple cutaneous, and in women uterine, leiomyomas exhibiting some distinctive features seen in this particular lesion; mainly cytoplasmic eosinophilic globules (Figure 2), nuclei with powdery chromatin exhibiting prominent nucleoli (Figure 3). Uterine examples tend to show similar albeit more pronounced nuclear features in addition to Hemangiopericytoma-like (HPC-like) vasculature, nuclear periodicity among other unique characteristics. Likewise, renal cell carcinomas arising in the context of HLRCC have their own set of distinct features including similar powdery chromatin and large nuclei with viral-like macronucleoli. These renal tumors were historically classified as type II papillary renal cell carcinomas (RCCs) or unclassifiable RCCs. The absence of the normal enzyme can be demonstrated by immunohistochemistry for Fumarate Hydratase (FH), which will show loss of staining in the lesional cells like in our case (Fig 4). In addition, one could performed immunohistochemistry for the abnormal product of the mutated FH gene (2-Succinocysteine, 2SC) a test that is not widely available.
Option A corresponds to the Birt-Hogg-Dubé syndrome (BHD, 17p11.2, OMIM 135150 )
Option B corresponds to the basal cell carcinoma (Gorlin, Gorlin-Goltz) syndrome (PTCH1, 9q22.32, OMIM 109400)
Option C describes hereditary paraganglioma pheochromocytoma syndrome, type 4 (SDHB, 1p36.13, OMIM 115310)
References
- Patel VM et al. Hereditary leiomyomatosis and renal cell cancer syndrome: An update and review. J Am Acad Dermatol. 2017 Jul;77(1):149-158. doi: 10.1016/j.jaad.2017.01.023. Epub, 2017 Mar 14.
- Buelow B et al. Immunohistochemistry for 2-Succinocysteine (2SC) and Fumarate Hydratase (FH) in Cutaneous Leiomyomas May Aid in Identification of Patients with HLRCC (Hereditary Leiomyomatosis and Renal Cell Carcinoma Syndrome). Am J Surg Pathol. 2016 Jul;40(7):982-8. doi: 10.1097/PAS.0000000000000626.
Case contributed by: Carlos Prieto Granada, M.D., Assistant Professor, Anatomic Pathology