Case History
Patient history:
80-year-old female underwent biopsy for a 4.5 cm ulcerated mass in the sigmoid colon, followed by low anterior resection.
What is the diagnosis?
- Sessile serrated adenoma/lesion
- Traditional serrated adenoma
- Tubulovillous adenoma
- Hyperplastic polyp
Answer: B, Traditional serrated adenoma
Discussion:
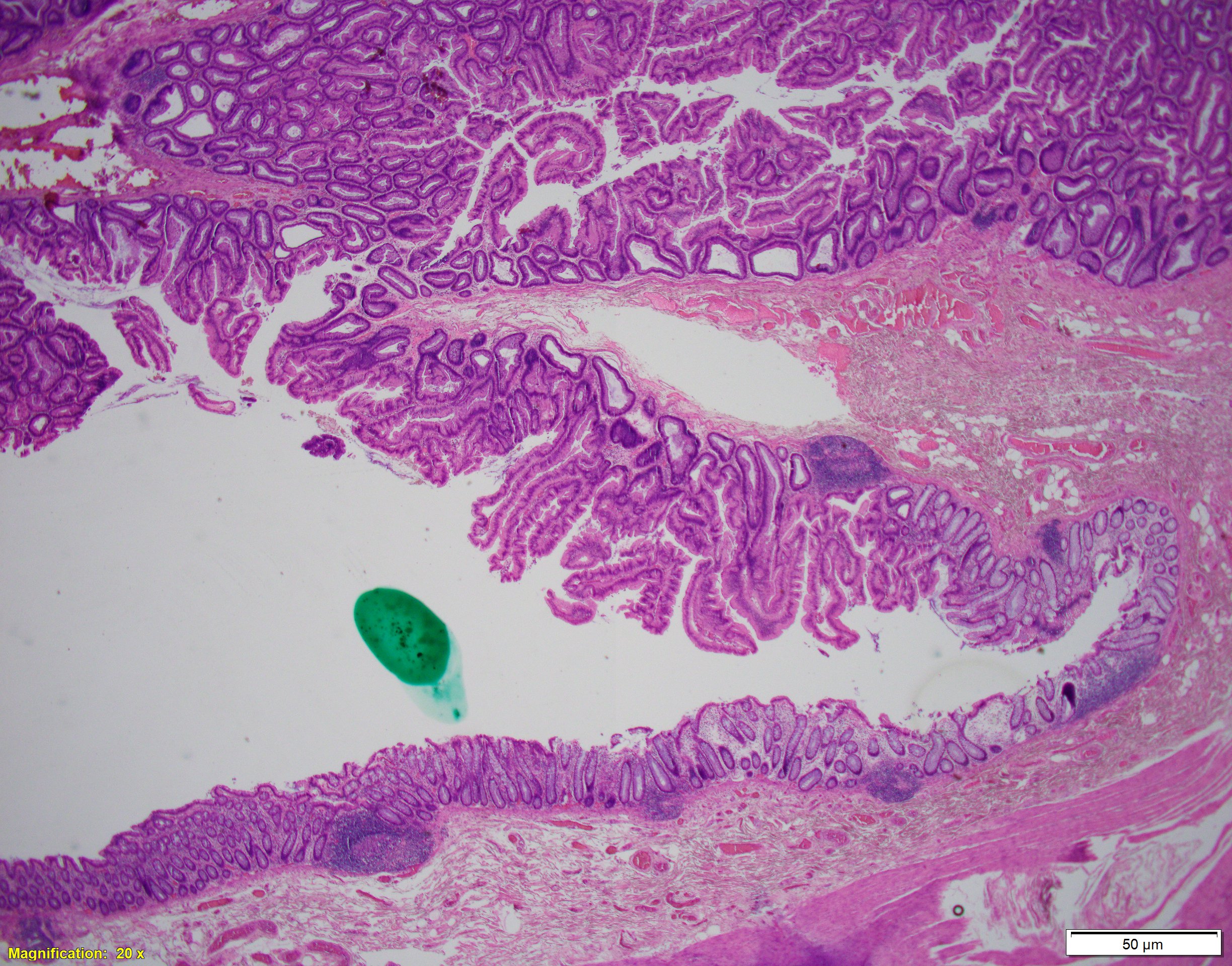
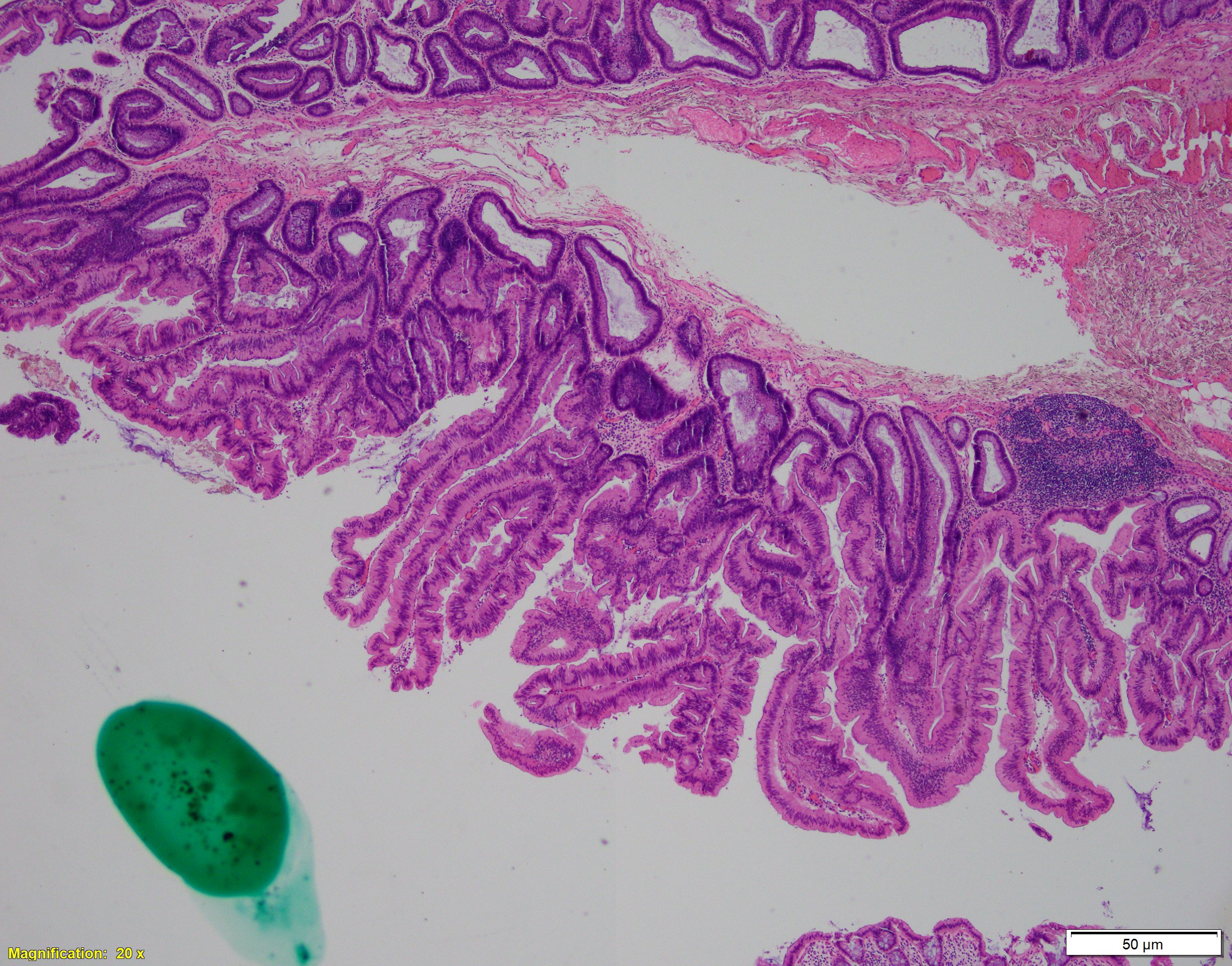
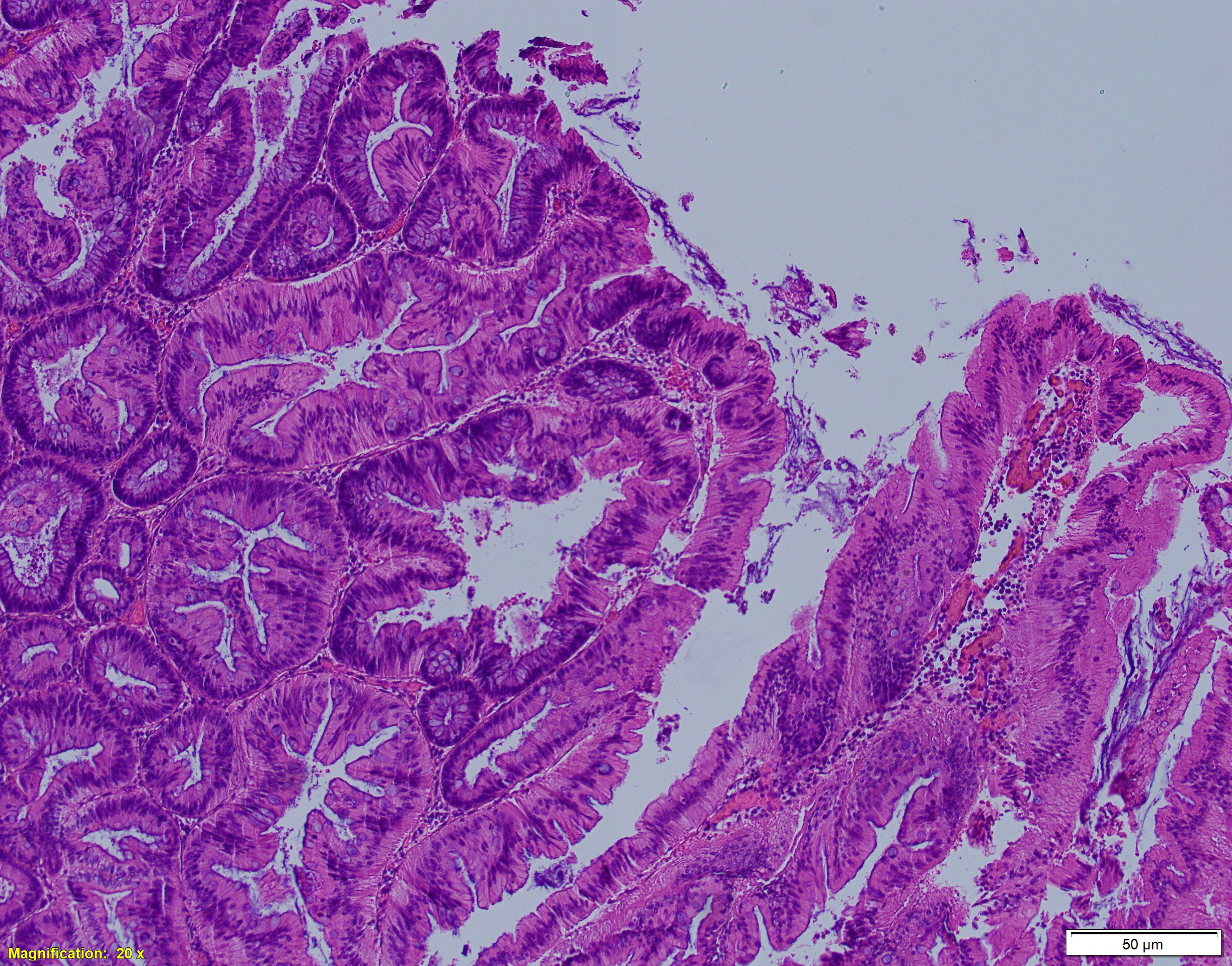
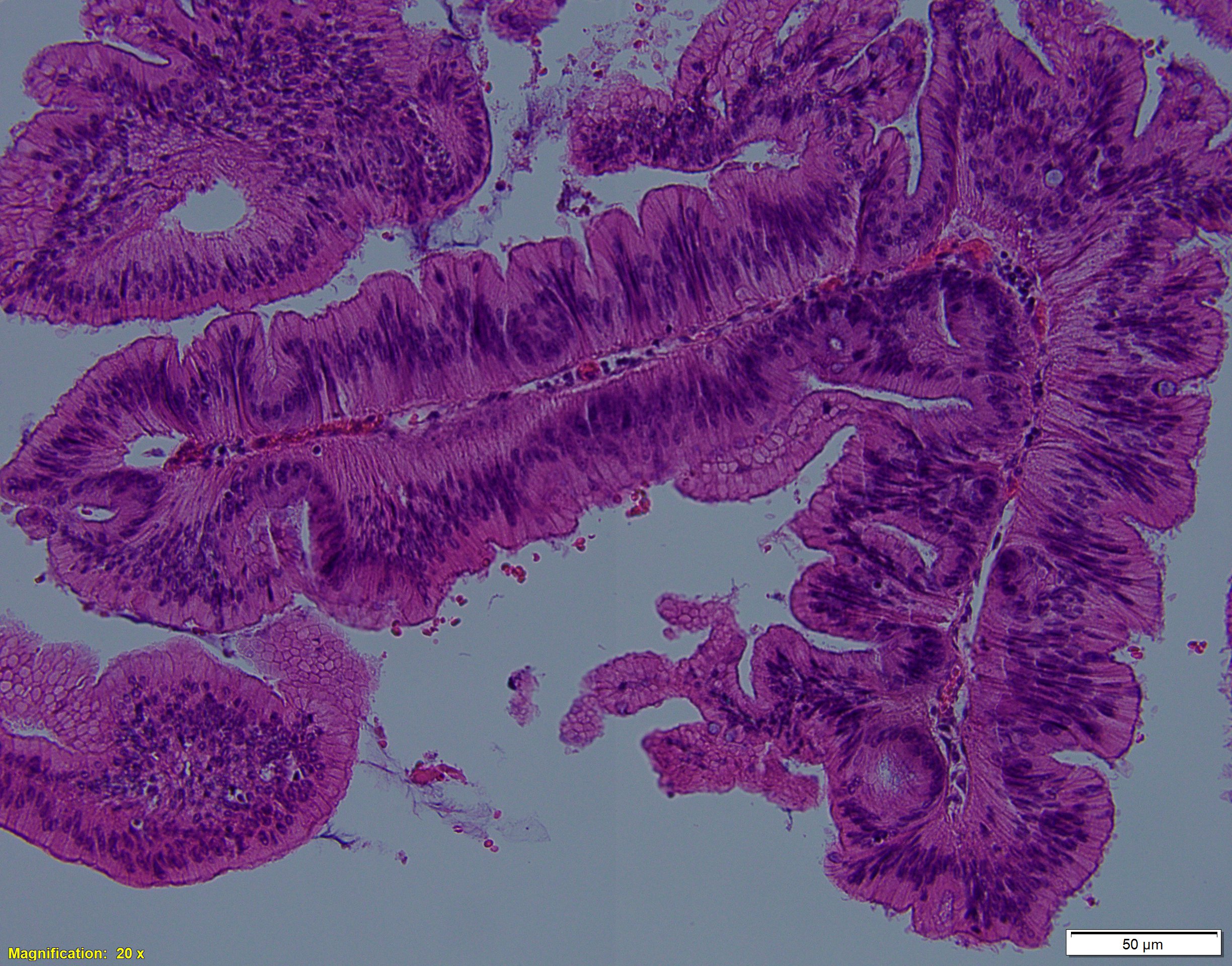
Traditional serrated adenoma is a serrated lesion, often associated with high grade dysplasia or invasive adenocarcinoma. It constitutes for 1-2% of colorectal adenomas and is mostly found in the left colon of elderly patient (mean age of 63 years). Endoscopically, it can present as large protuberant polyp in the distal colorectum or as flat lesion in the proximal colon; it is usually larger than 1cm in size. Morphologic findings include prominent, slit-like serration of glands within the polyp with complex architecture (infolding, budding, and papillary tufting). The lesion consists of tall/columnar neoplastic cells with hypereosinophilic cytoplasm with crowded pseudostratified ad elongated (“pencillate”) nuclei. Another characteristic feature is an ectopic crypt formation (small “budding”crypts). Cytologic dysplasia can be recognized by lack of surface maturation, immature goblet cells, and multiple upper zone mitoses. On the molecular level, traditional serrated adenoma most frequently harbor KRAS mutations, although BRAF mutations, as well as MSI, CIMP had also been reported. Differential diagnosis includes tubular/tubulovillous adenoma, which is by far the most common type of colorectal adenomas, as well as sessile serrated adenomas.
Case contributed by: Sophia Sher, M.D., Fellow, GI Pathology