Case History
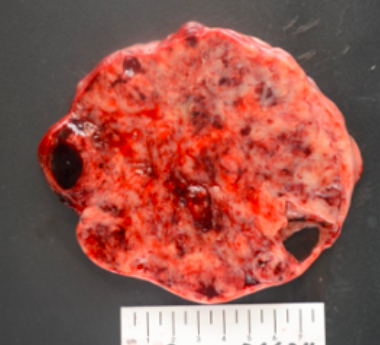
18 year-old female with 2 weeks of pelvic pain. CT showed a heterogeneous pelvic mass measuring 12.8 x 11.1 cm.CA-125 was 129 and AFP and beta-hCG (UPT negative) were not measured. She underwent right salpingo-oophorectomy. The ovary/mass measures 16.5 x 12 x 9.6 cm. Serially sectioning reveals a solid and partially cystic (90% solid, 10% cystic), variegated, homogenous, soft mass with punctate areas of hemorrhage. The fallopian tube grossly was not involved. Right external iliac and periaortic lymph nodes were involved by tumor. See below for the gross and microscopic photos of the ovary. The tumor cells show focal immunoreactivity for Pankeratin cocktail, AE1, AE3, Cam5.2 and 34BE12, patchy dot-like positivity with EMA, patchy and strong immunoreactivity for WT1 and SALL4, patchy immunoreactivity for Synaptophysin, focal positivity for Calretinin and CD10. Chromogranin and CD56, PAX8, OCT3/4, CD30, Inhibin, SF1, CD45, Desmin, GFAP and Sox10 were all negative in the tumor cells. INI1 expression was retained. What is the diagnosis?
What is the diagnosis?
- Juvenile granulosa cell tumor
- Dysgerminoma
- Large cell variant of small cell carcinoma of the ovary, hypercalcemic type
- Sex-cord stromal tumor
Discussion:
Small cell carcinoma of the ovary, hypercalcemic type, is an undifferentiated tumor composed of small cells, with or without a large cell component, often associated with hypercalcemia, unrelated to small cell neuroendocrine (pulmonary) carcinoma.
This tumor is rare, occurs almost exclusively in women of reproductive age and children (median: 25 years). Tumors are usually large, solid, fleshy and tan to white to grey, often with hemorrhage, necrosis and cystic degeneration.
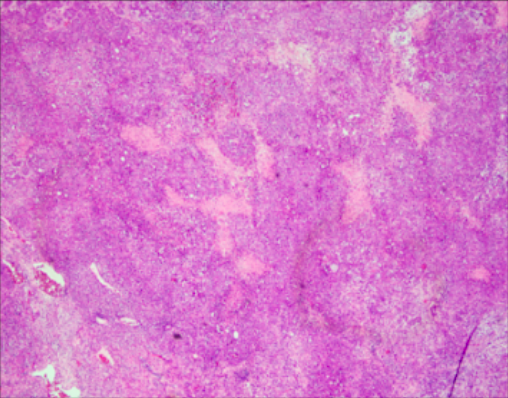
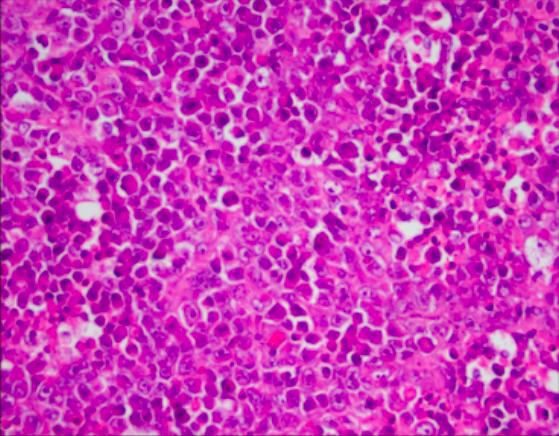
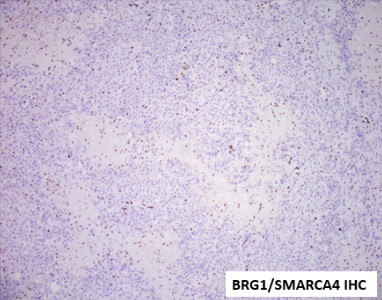
Tumor cells grow in sheets, nests, cords, and trabeculae. Scattered follicle like spaces with eosinophilic or basophilic secretions are often seen. Cells have monomorphic round, ovoid or occasionally spindles nuclei with vesicular chromatin, small nucleoli, scant cytoplasm, and brisk mitotic activity. Large cells are present in half of these tumors, which are designated “small cell carcinoma, large cell variant” if the large cells are predominant. Immunohistochemistry reveals absence of SMARCA4 (and SMARCA2) in almost all tumors, along with diffuse expression of WT1, p53, and p16 and variable expression of claudin-4, SALL4, keratins, EMA (especially in the large cell component), CD10, calretinin, and all neuroendocrine markers. Inhibin and TTF1 are negative. Prognosis is poor.
Reference:
Female Genital Tumors, WHO classification of Tumours, 5th Edition.