Case History
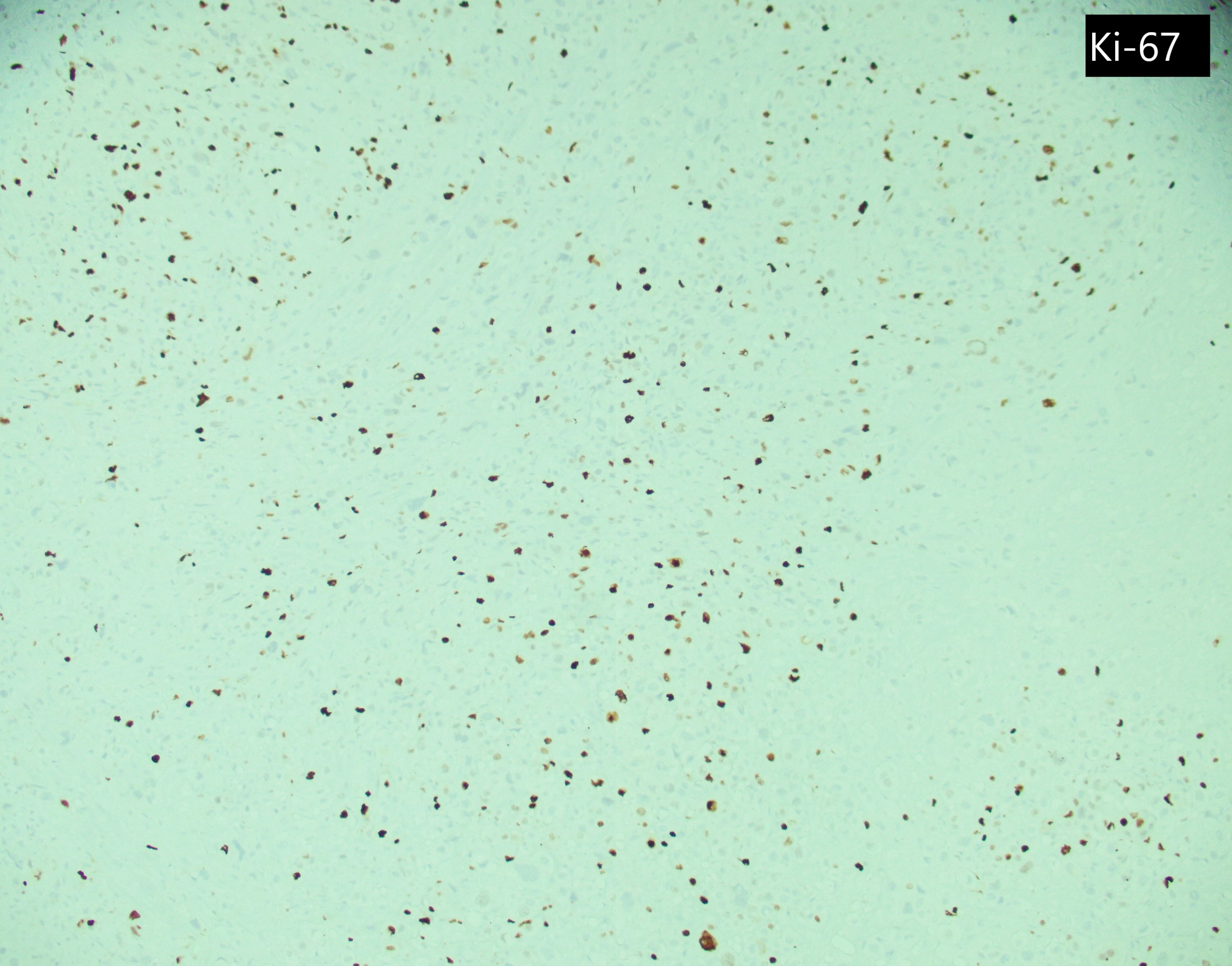
A 19-year-old female with a pregnancy c/b pre-eclampsia. She has had persistent bleeding for 4 months since her delivery. U/S showed a 5 cm endomyometrial mass. Her serum HCG was 161 mIU/mL. D&C showed neoplastic cells which are GATA3+, p63-, and has a Ki67 PI of 30%.
What is the diagnosis?
- Exaggerated placental site
- Gestational Choriocarcinoma
- Placental Choriocarcinoma
- Epithelioid trophoblastic tumor
Answer: C. Placental site trophoblastic tumor
Discussion
Placental site trophoblastic tumor (PSTT) is a malignant neoplasm of implantation site intermediate trophoblasts. Two third of the cases follow a full-term pregnancy with a median latency of 12-18 months. The most common presentations are vaginal bleeding, enlarges uterus or history of missed abortion. Mild to moderate elevation of serum hCG (5-26,000 mIU/mL, average 680 mIU/mL) is detectable in 80% of cases.
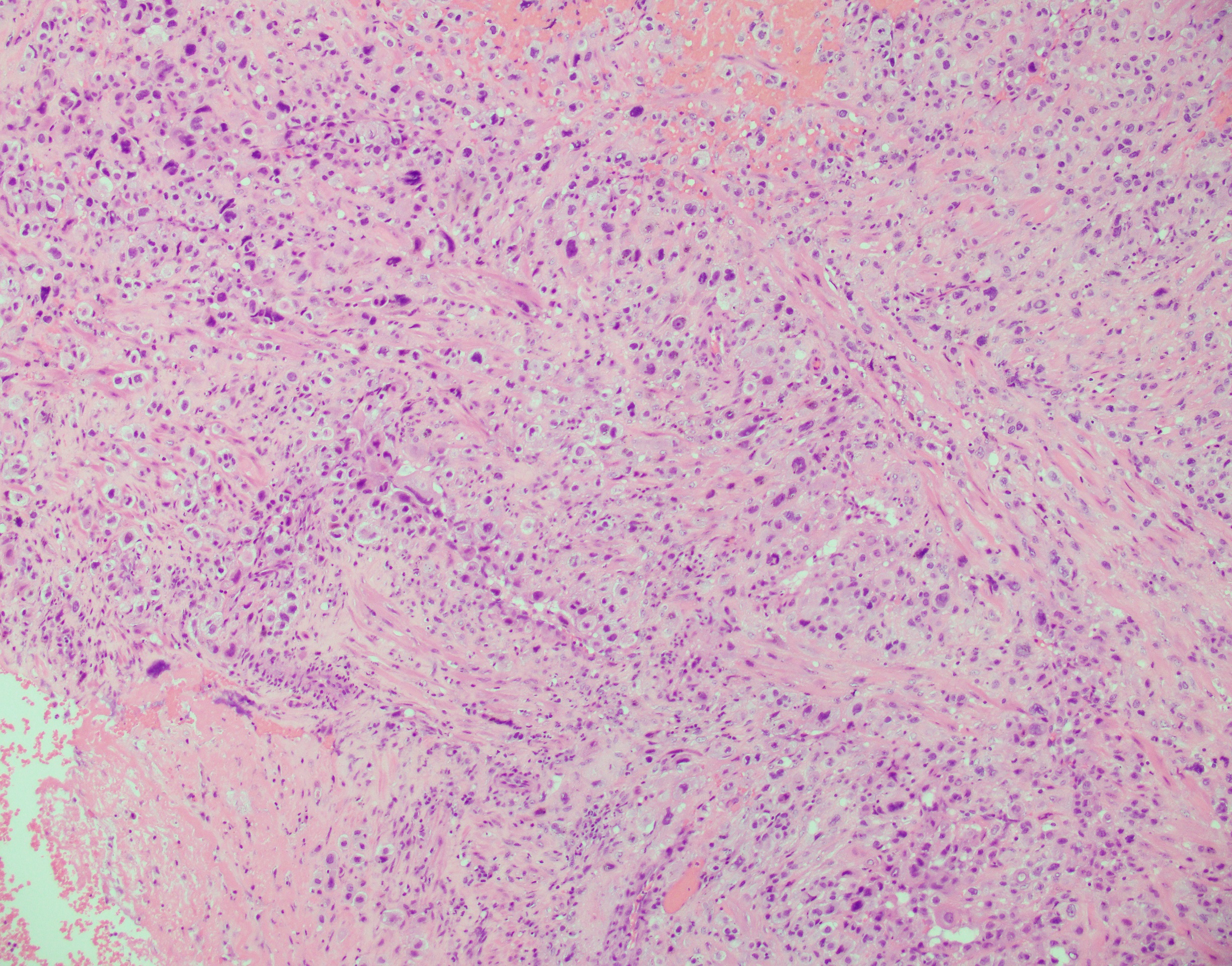
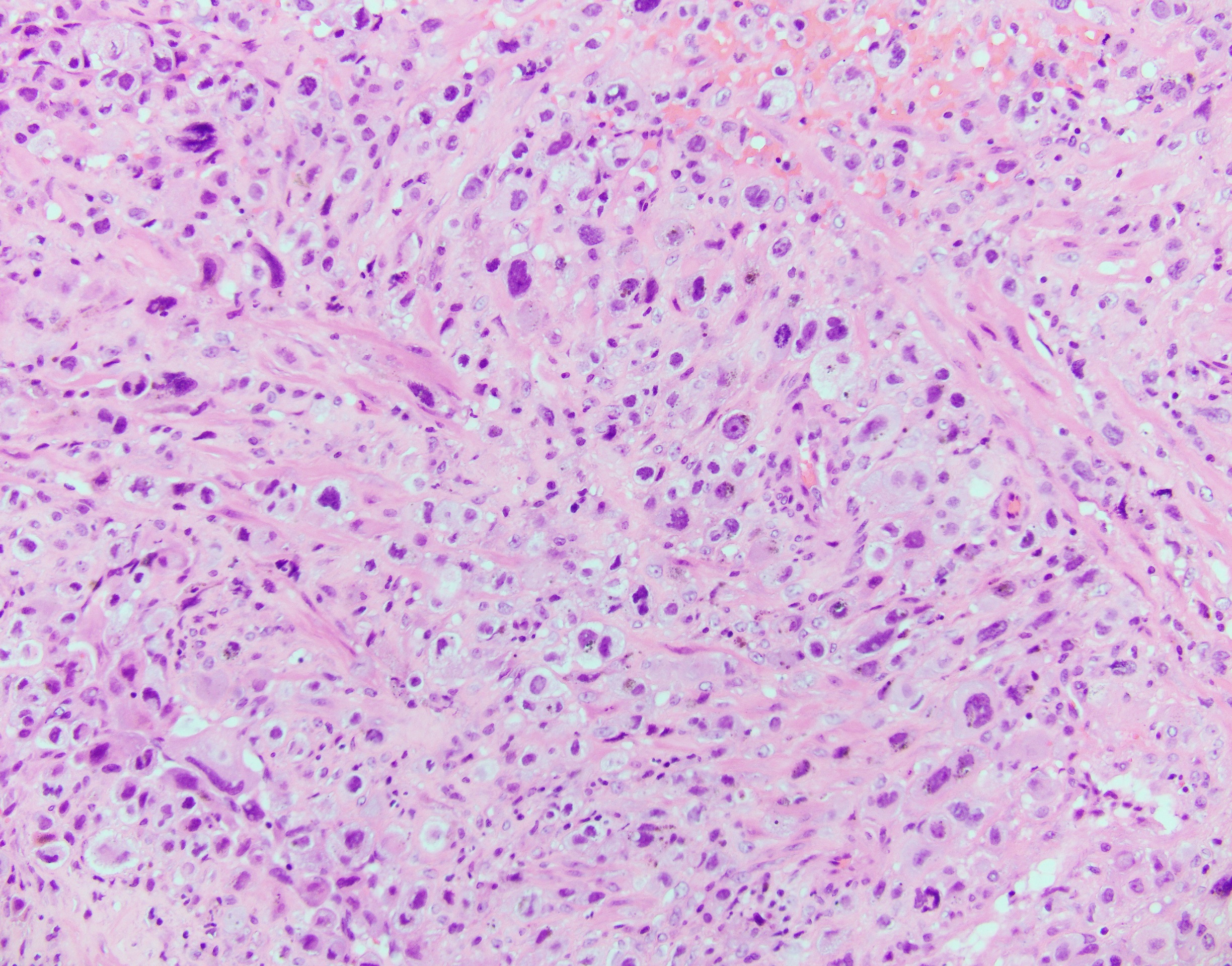
Histologically, the tumor has an infiltrative growth pattern consisting of aggregates or sheets of large, polyhedral to round, predominantly mononucleated cells, with scattered multinucleated cells. The tumor typically infiltrate the myometrium by separating the smooth muscle cells. The cells usually have abundant amphophilic and occasionally eosinophilic or clear cytoplasm. Nuclei are pleomorphic with atypia, large, convoluted and marked hyperchromasia. Most tumors have low mitotic activity. Charactaristic vascular invasion is often present, where tumor cells replace the vessel wall of myometrial vessel.
Top differential diagnosis include exaggerated placental site (EPS), epithelioid trophoblastic tumor (ETT) and gestational choriocarcinoma. EPS would show Ki67 proliferation index 1-5%. ETT has similar histologic features on H&E but stains diffuse positive for p63. Gestational choriocarcinoma would show a Ki67 proliferation index >90%.
Simple hysterectomy is curative in most cases. However, approximately 25-30% of patients may develop recurrent disease or metastasis. Mortality rate is 6.5-27%. Poor prognostic features include tumor cells with clear cytopalasm, deep myometrial invasion, large tumor size, necrosis, high mitotic rate (>5 mitosis/10 HPF), > 48 months since antecedent pregnancy, age >40 years.
Selected references:
1.Placental site trophoblastic disease, WHO Classification of Tumors, Female Genital Tumors 5TH edition.