Case History
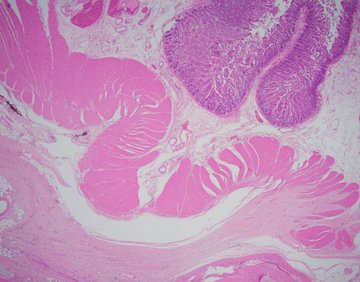
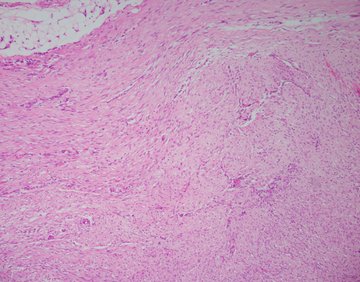
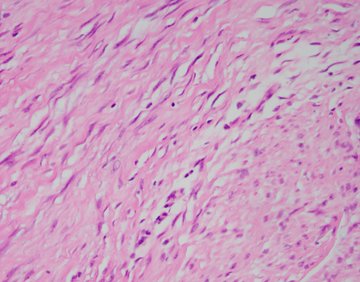
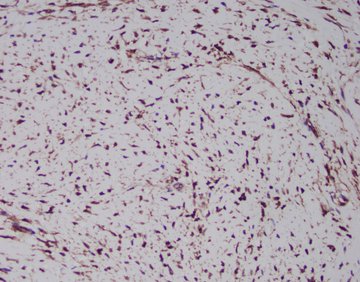
A 34-year-old male presents to the emergency department with abdominal pain. Imaging shows a circumfrential mass causing obstruction of the small bowel. Sections of the mass (H&E shown below) show a mesenteric based spindle cell proliferation with long sweeping fascicles, small blood vessels, bland cytology, no mitoses or necrosis. Immunohistochemical stain for beta catenin shows nuclear positivity in the lesional cells (IHC shown below), and they are negative for desmin, S100, CD117, and SOX10.
What is the diagnosis?
A. Gastrointestinal stromal tumor (GIST)
B. Leiomyoma
C. Desmoid fibromatosis
D. Schwannoma
Discussion:
Desmoid fibromatosis can also be referred to as desmoid-type fibromatosis, abdominal/mesenteric fibromatosis, aggressive fibromatosis or desmoid tumor. These terms refer to intra-abdominal fibromatosis that arises from the mesentery, most commonly of the small bowel followed by ileocolic or mesocolon. Other sites may include pelvis, omentum, or retroperitoneum. These masses are usually painless, slow growing and can become quite large. They can be detected incidentally on abdominal imaging. Sometimes the mass can cause bowel obstruction. Approximately half of the cases are associated with prior surgical procedure or trauma.
Grossly, the lesions are firm with tan-white cut surfaces, often located in the mesentery of small bowel or colon. Histologic sections usually show a low-grade spindle cell proliferation in long sweeping fascicles. Small blood vessels often show perivascular edema. Desmoid fibromatosis should be included in the differential for a spindle cell lesion in the gastrointestinal tract. Other differential diagnoses includes gastrointestinal stromal tumor (GIST), leiomyoma, inflammatory myofibroblastic tumor (IMT), schwannoma, or nodular fasciitis.
Immunohistochemical stains can help differentiate between these. Nuclear staining with beta-catenin is the most helpful stain to confirm desmoid fibromatoses. The other differential diagnoses may show cytoplasmic staining but not nuclear staining. Desmoid fibromatosis may show smooth muscle actin or focal desmin positivity, like leiomyoma, however leiomyoma will not show nuclear beta-catenin staining. Desmoid fibromatosis should be negative for C-kit and DOG1 (positive in GIST), S100 (positive in schwannoma) and ALK (positive in IMT).
Most cases of desmoid fibromatosis are sporadic and have activating mutations in CTNNB1 gene which is detected by the nuclear beta-catenin immunohistochemical stain. Approximately 10% of cases have a germline inactivating mutations in APC gene, associated with familial adenomatous polyposis. Prognosis is typically good as these tumors are considered benign, although they may locally recur.
References:
WHO Classification of Tumours Editorial Board. Digestive system tumours [Internet]. Lyon (France): International Agency for Research on Cancer; 2019 (WHO classification of tumours series, 5th ed.; vol. 1). Available from: https://tumourclassification.iarc.who.int/chapters/31.
Contributed by Anne Prater, D.O., Surgical Pathology Fellow, UAB Pathology