Case History
A 36 y/o male, with hx of prior IVDU (HCV+) and new diffuse adenopathy, as well as an anterior and posterior mediastinal mass (7.7x6.5cm) extending through posterior abdominal wall with displacement and encasement of abdominal aorta and renal arteries. FNA of the chest and abdominal mass.
What is the diagnosis?
A. Adenocarcinoma
B. Melanoma
C. Germ cell neoplasm
D. SMARCA4/BRG1-deficient non-small cell carcinoma
The answer is “C”, germ cell neoplasm
Discussion
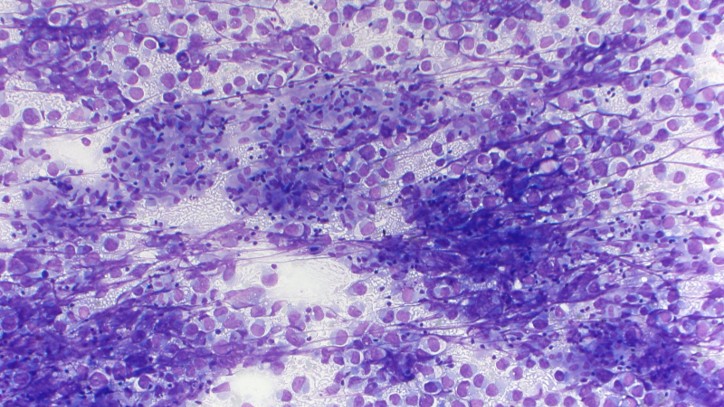
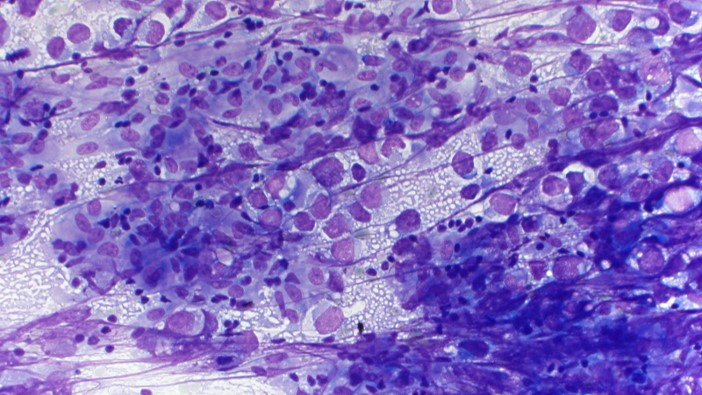
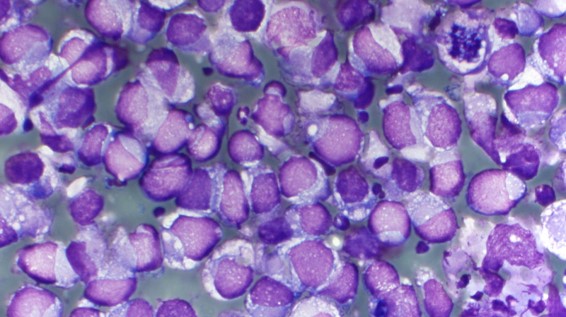
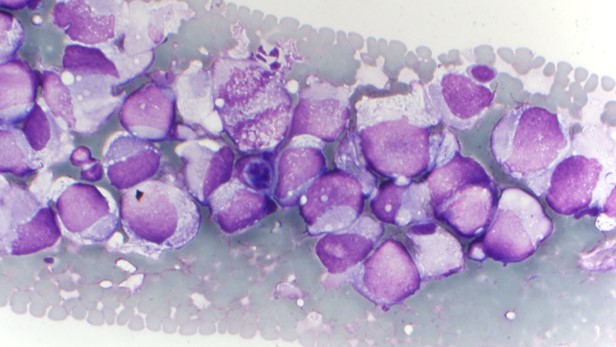
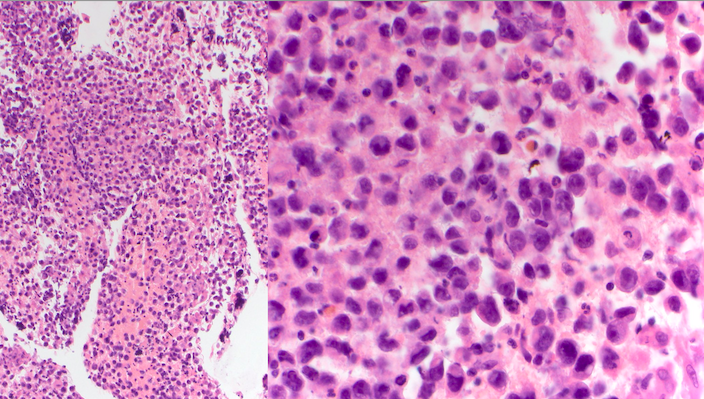
The specimen is cellular and consists of abundant large and dyshesive cells with somewhat rhabdoid/plasmacytoid morphology, prominent nucleoli, and moderate amounts of vacuolated cytoplasm. In the background there are small lymphocytes and a focal bubbly/tigroid appearance, as well as non-necrotizing granulomas.
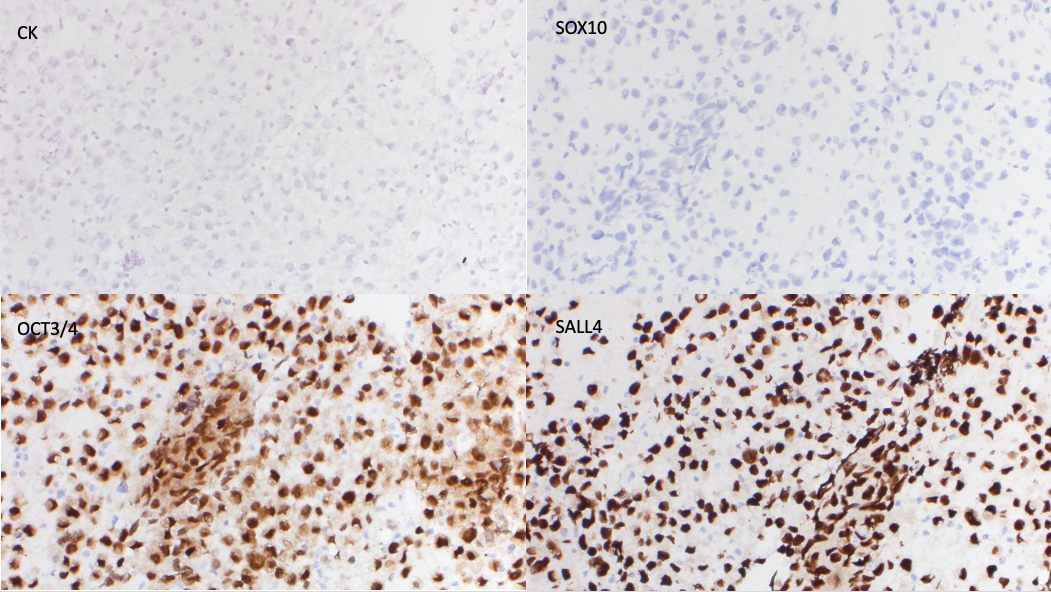
Immunohistochemical stains were performed on this case. The cells were positive for OCT3/4 and SALL4, and negative for cytokeratin cocktail, SOX10, INI1 (retained), and SMARCA4 (retained). Together with the morphology, this staining pattern is consistent with germ cell neoplasm.
Germ cell tumors (GCTs) are classified as extragonadal if there is no evidence of a primary tumor in the testes or ovaries. Extragonadal GCTs typically arise in midline locations; in adults, the most common sites, in order of frequency, are the anterior mediastinum, the retroperitoneum, and the pineal and suprasellar regions. Based on morphology, they are typically divided into seminomas versus nonseminomatous GCTs (teratomas [mature or immature], embryonal carcinomas, yolk sac tumors and choriocarcinoma) The two key issues in establishing the diagnosis are the exclusion of metastasis from a primary testicular GCT and distinguishing from another type of poorly differentiated tumor. This patient underwent a subsequent radical orchiectomy that showed testicular parenchyma with marked tubular atrophy, hyalinosis, scarring, focal dystrophic calcifications, hemorrhage, Sertoli cell adenomas, and hyperplastic Leydig cells, suggestive of regressed germ cell tumor.
Contributed by Frida Rosenblum, M.D., Associate Professor, Anatomic Pathology