Case History
A 16-year old female presents with abnormal uterine bleeding. A 3.5 cm submucosal leiomyoma is clinically suspected, and she underwent a hysteroscopic myomectomy.
What is the most likely diagnosis?
B. Atypical polyploid adenoma
C. Benign adenomyomatous polyp
D. Benign endometrial polyp
Answer: (A) Müllerian adenosarcoma
Müllerian adenosarcomas (MA) are rare, biphasic tumors composed of a benign epithelial component and malignant stromal component. In contrast to the more well known carcinosarcoma, the malignant stromal component of MA show low-grade atypia. These tumors can present in the uterine corpus, vagina, or cervix, and may be extrauterine in origin, arising in a background of endometriosis. Patients presenting with these malignancies are normally peri- or postmenopausal with less than 30 cases reported of these tumors presenting in adolescent females.
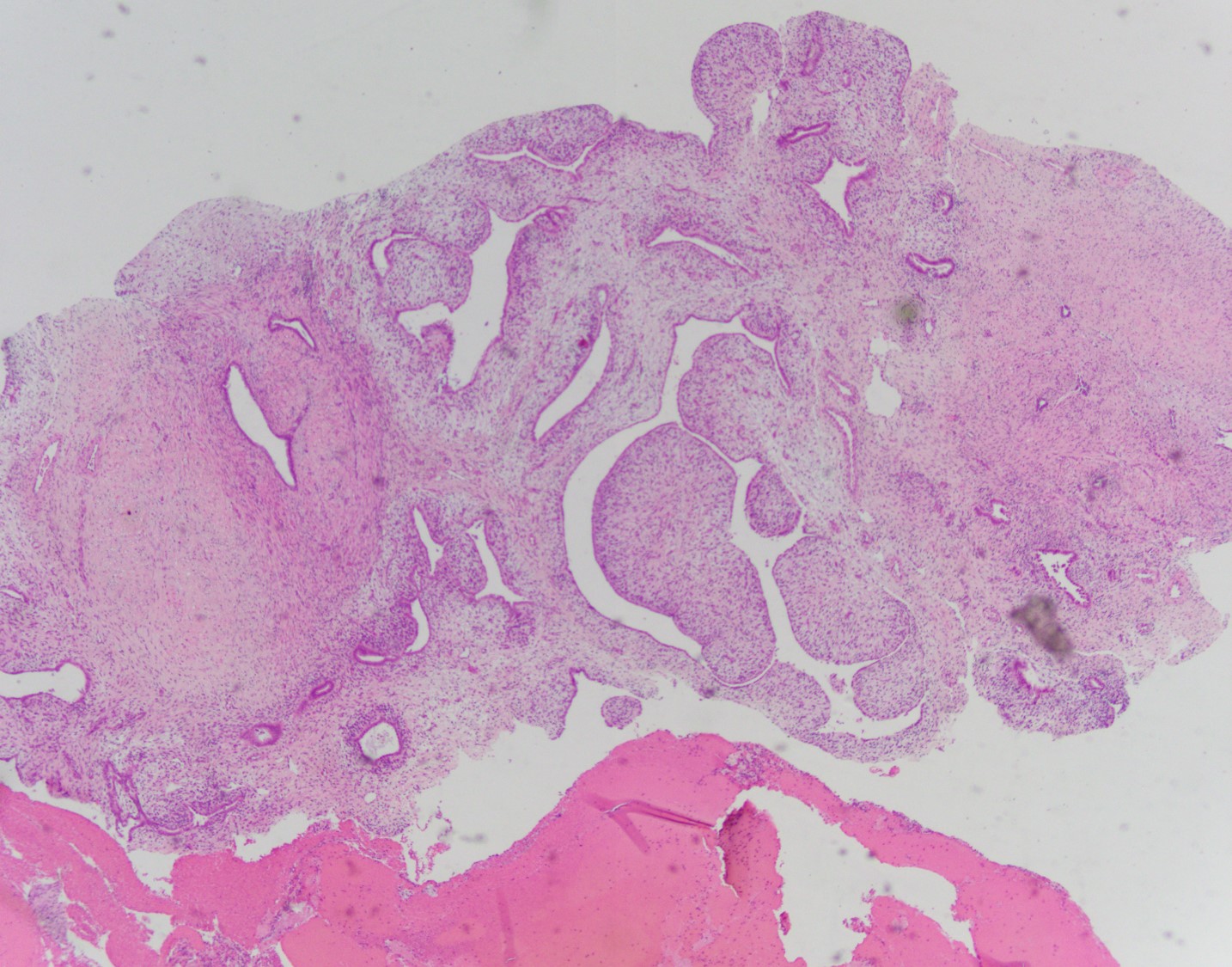
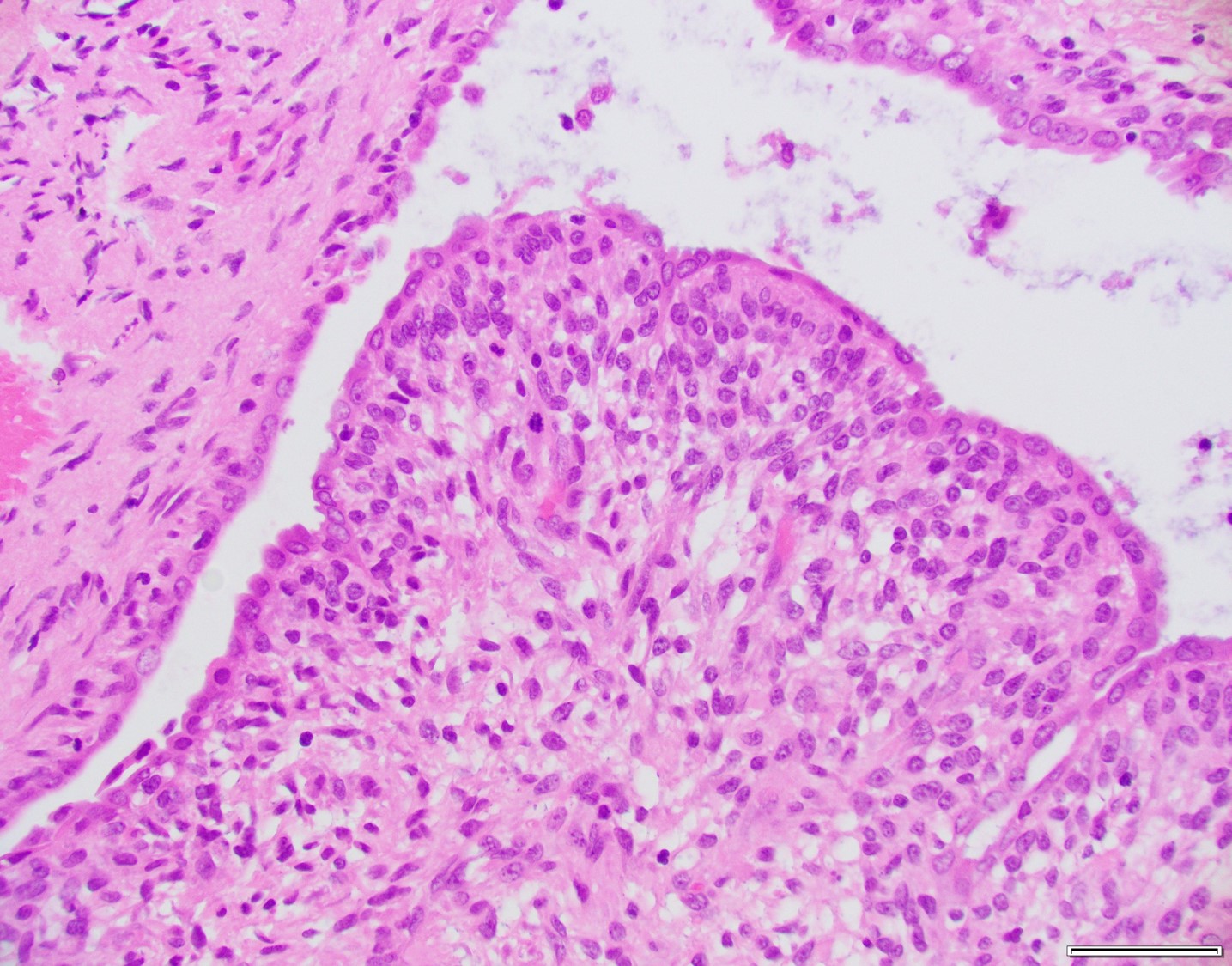
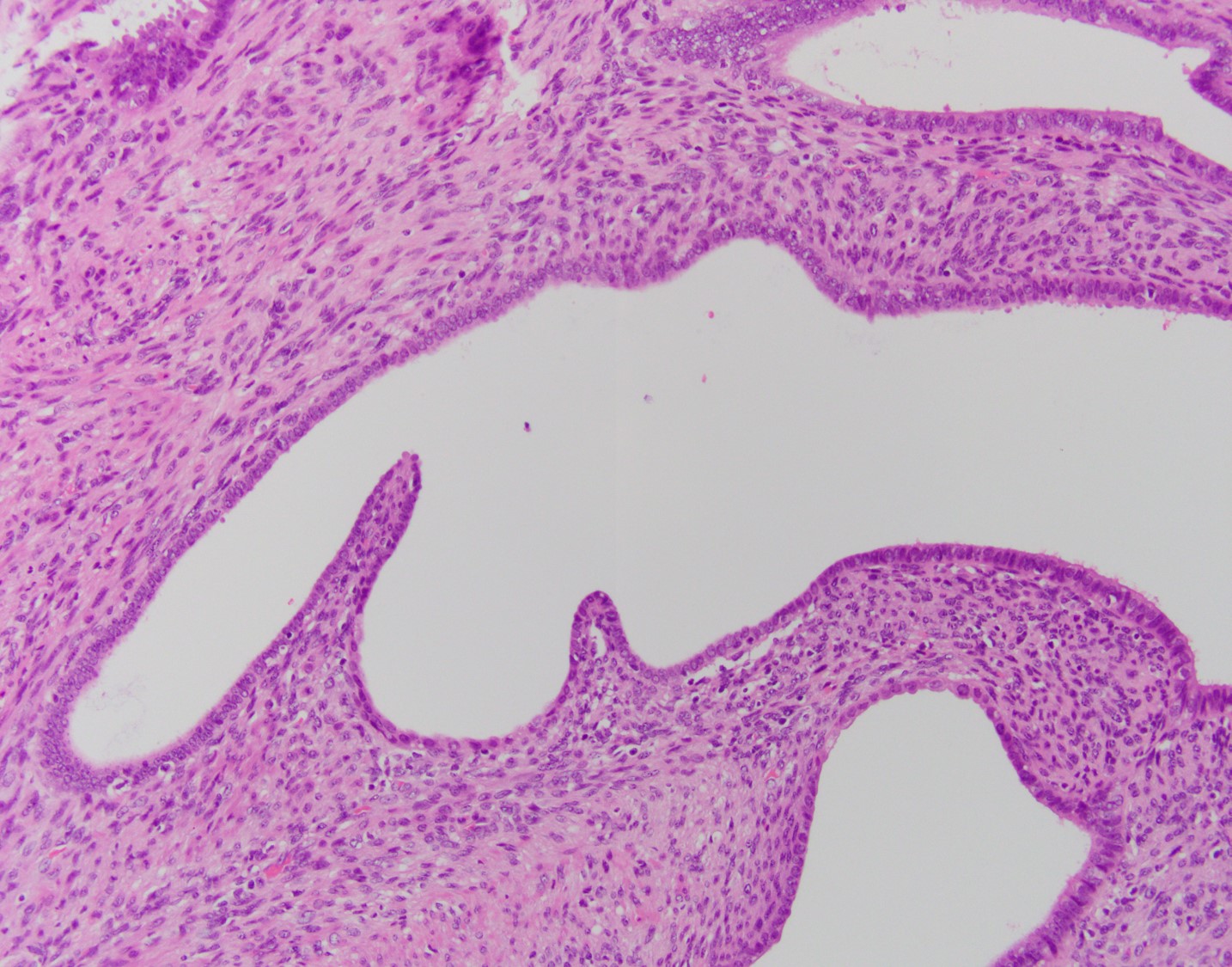
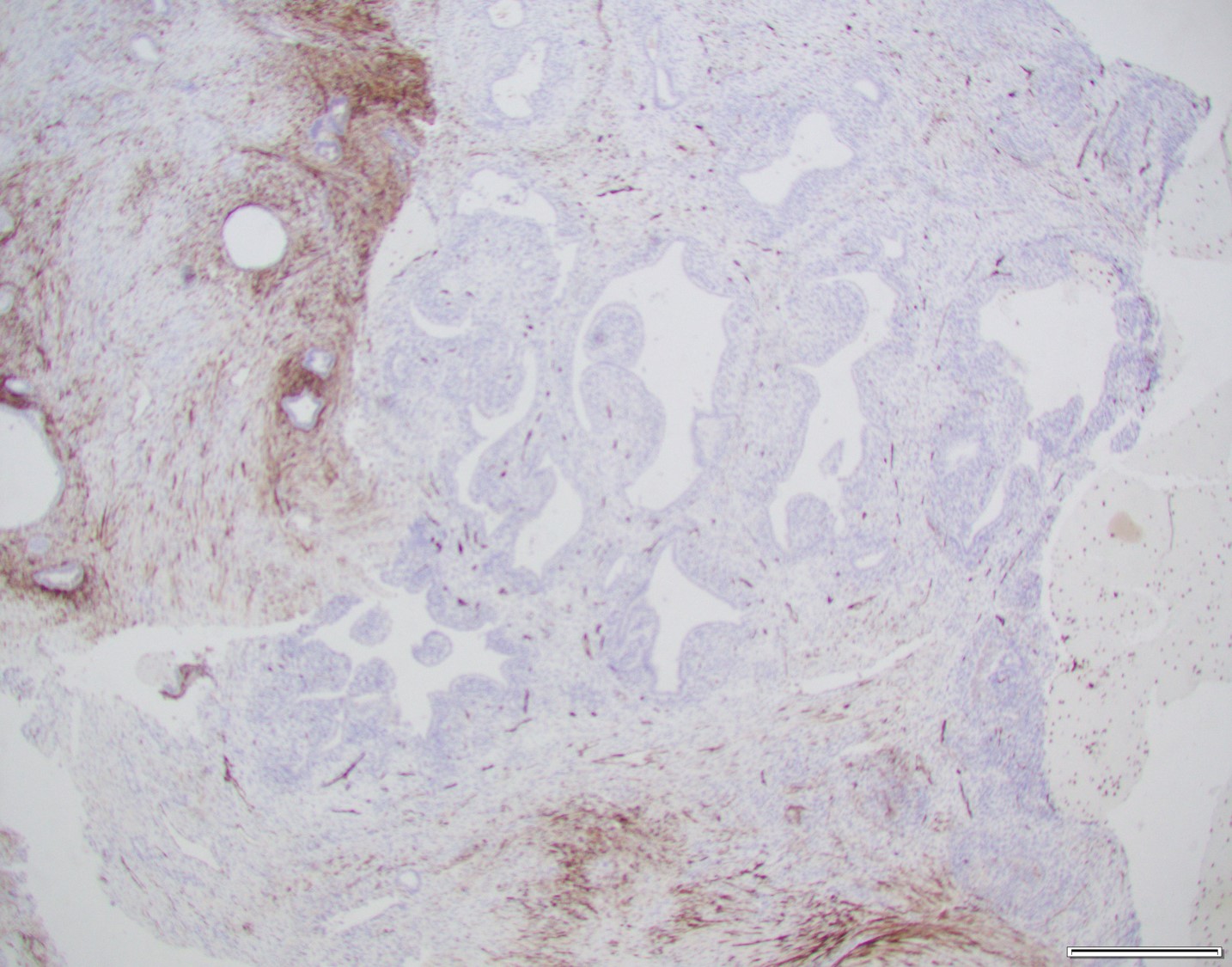
Histologically, MA usually have a phyllodes-type pattern with dilated glands lined by benign endometrial or ciliated epithelium surrounded by a distinct cuff of neoplastic stroma. This stroma is normally hypercellularand can have subtle atypical features. These tumors are often positive for CD10, ER, and PR, however there have been a subset of cases that are negative for CD10.
There are two components comprising this specimen, which are focally intimately associated with one another. The first component consists of endometrial glands and stroma surrounded by smooth muscle bundles, which in the proper clinical setting could represent a benign adenomyomatous polyp. The second component consists of a biphasic process of benign glands and stroma with a phyllodes-like architecture. The stroma surrounding the glands shows periglandular "cuffing" with very low-grade atypia. There is increased mitotic activity (greater than 2 mitoses/10 HPF) in the areas with the phyllodes-like architecture. Immunohistochemical staining showed two distinct staining patterns in the two components. The adenomyomatous polyp component showed CD10 highlighting endometrial stroma in the adenomyomatous areas with surrounding smooth muscle bundles positive for caldesmon and desmin while the stroma in the phyllodes-like area was positive for desmin and caldesmon but was negative for CD10. The patient was treated with a hysterectomy, where there was minimal focal residual disease identified.