Case History
80-year-old female with post-menopausal bleeding and 5.5 cm polypoidal mass in the endometrium.
What is the best diagnosis?
- Endometrial stromal sarcoma
- Serous carcinoma
- Mixed Mullerian tumor/carcinosarcoma
- Leiomyosarcoma
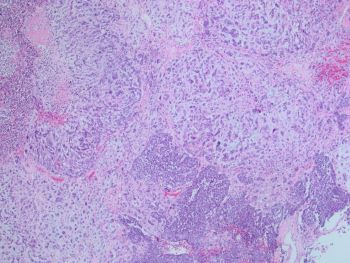
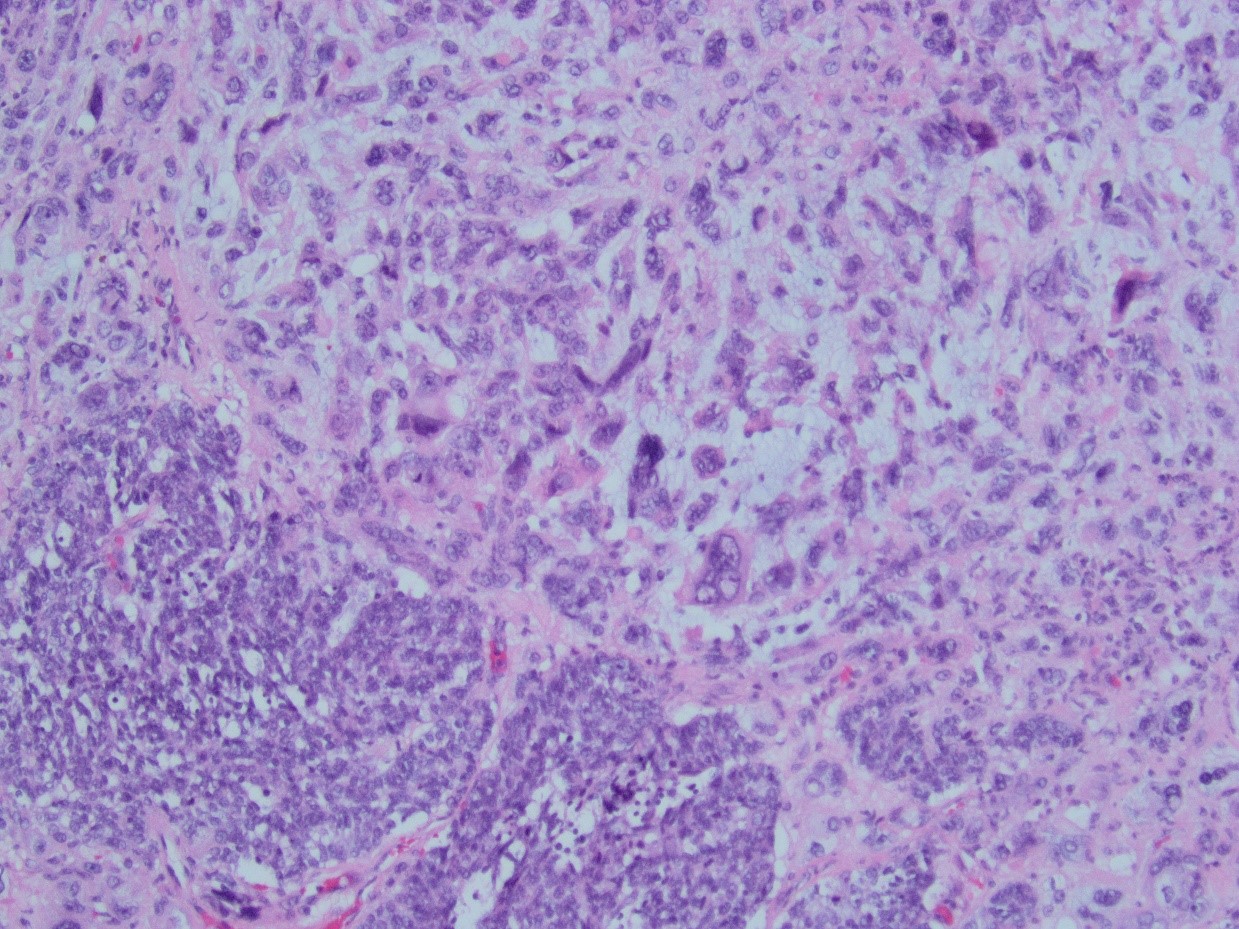
Answer: C. Mixed Mullerian tumor/carcinosarcoma. Sections from the tumor show biphasic, malignant tumor with high-grade epithelial and sarcomatous components consistent with carcinosarcoma.
Clinical features: Patients usually present with vaginal bleeding, uterine enlargement, or a pelvic mass.
Macroscopic appearance: Usually present as large, polypoid mass, usually filling the uterine cavity. Areas of hemorrhage, necrosis and cystic degeneration are frequent.
Histopathology: The tumors are composed of an admixture of malignant epithelium and mesenchyme, which is typically sharply juxtaposed. The carcinomatous component often shows endometrioid or serous differentiation, but clear cell and undifferentiated carcinoma may be encountered. The mesenchymal component most commonly consists of high-grade sarcoma NOS, but heterologous elements (including rhabdomyosarcoma, chondrosarcoma, and rarely osteosarcoma) may be seen
Essential and desirable diagnostic criteria
Essential: high-grade malignant epithelial and mesenchymal components.
Desirable: in rare cases, immunohistochemistry can be helpful in confirming specific mesenchymal differentiation (e.g. rhabdomyoblastic).
Prognosis and prediction
Patients with FIGO stage I–II disease have a 5-year disease-specific survival rate of 60%, while patients with stage III and IV disease, respectively, have rates of 25% and 10% In addition to an advanced stage, other independent factors associated with poor prognosis are size > 5 cm, myometrial invasion > 50%, lymphovascular invasion, and sarcoma predominance. Some large recent series suggest that serous histology and heterologous rhabdomyoblastic differentiation are significantly associated with worse survival.
Reference: WHO classification of Female genital tumors. 5th edition.