Case History
A female in her seventies presented with an 8 cm mass in the gastric body. A partial gastrectomy was performed. Representative H&E and IHC images are below.
What is the diagnosis?
- Gastric adenoma, foveolar type
- Gastric adenoma, pyloric gland type
- Gastric adenoma, intestinal type
- Gastric adenoma, oxyntic gland type
The correct answer is B: Gastric adenoma, pyloric gland type.
Discussion: Per WHO Classification of Tumours Editorial Board: Digestive System Tumours 2019, Gastric adenomas are polypoid lesions consisting of gastric dysplastic/neoplastic epithelium and their classification is associated with epithelial phenotypes such as pyloric gland type, intestinal type, foveolar type, and oxyntic gland type.
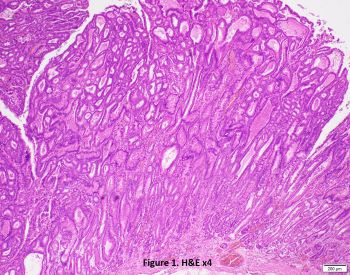
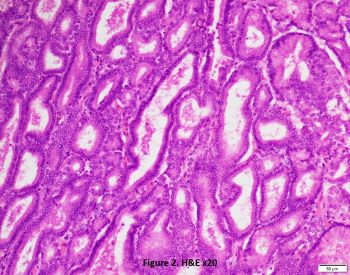
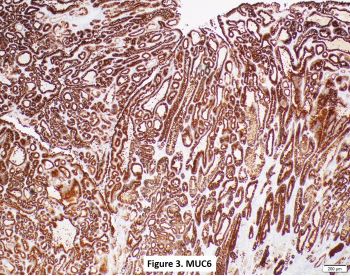
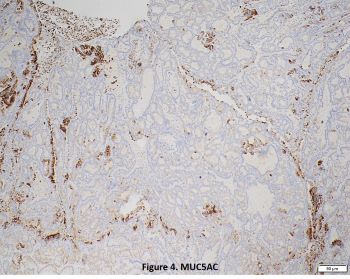
Gastric pyloric gland adenomas (PGAs) mainly develop from chronic atrophic gastritis (e.g., autoimmune gastritis) and syndromic setting (e.g., FAP). PGAs are polypoid lesions or masses with an average size of 2 cm (range: 0.3–10 cm). Microscopically (Figures 1 and 2) the lesion is composed of closely packed uniform glands lined by bland uniform cuboidal/low columnar epithelium with pale to eosinophilic cytoplasm. The nuclei are round-to-ovoid and basally-located. High-grade dysplasia (HGD) is observed in 40-50% of PGAs; adenocarcinoma (AdC) is observed in almost half of all cases. However, submucosal invasion does not exceed 10%. Diffuse MUC6 positivity by IHC is the hallmark of pyloric gland differentiation (Figure 3) with variable MUC5AC staining (Figure 4). Because of the relatively high risk of HGD/AdC, complete resection is mandatory.
Foveolar-type adenomas are composed of atypical columnar or cuboidal foveolar epithelium with apical mucin cap, which can distinguish PGAs (lack of apical mucin cap) from foveolar-type adenoma. The adenomas demonstrate strong, diffuse MUC5AC expression with weak/focal MUC6 positivity.
Intestinal-type adenomas consists of dysplastic intestinalized epithelium. They are associated with intestinal metaplasia by H. pylori or autoimmune gastritis. Microscopically the lesions show the dysplastic tubules lined by columnar epithelium featuring intestinal differentiation in the form of elongated nuclei akin to those in colorectal adenomas with variable contributions of goblet cells and Paneth cells. Immunohistochemically the adenomas are positive for CDX2 and MUC2. This type is more prone to development of HGD/AdC than foveolar-type lesions.
Oxyntic gland adenomas (OGAs) are rare and recently recognized epithelial neoplasms composed of crowded glands/tubular fusion or irregular anastomosing cords of columnar cells with pale basophilic cytoplasm and mild nuclear atypia, mimicking the oxyntic glands (mainly chief cells). The adenoma cells are highlighted by pepsinogen I and H+/K+ ATPase IHC. MUC6 can be positive. Careful assessment of the submucosa is essential, because herniation through the muscularis mucosae is relatively common and should not be considered as evidence of invasion.
References:
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours of the Digestive System. 5th ed. Lyon: International Agency for Research on Cancer. 2019;328–30.
- Kővári B, Kim BH, Lauwers GY. The pathology of gastric and duodenal polyps: current concepts. Histopathology. 2021 Jan;78(1):106-124.