Case History
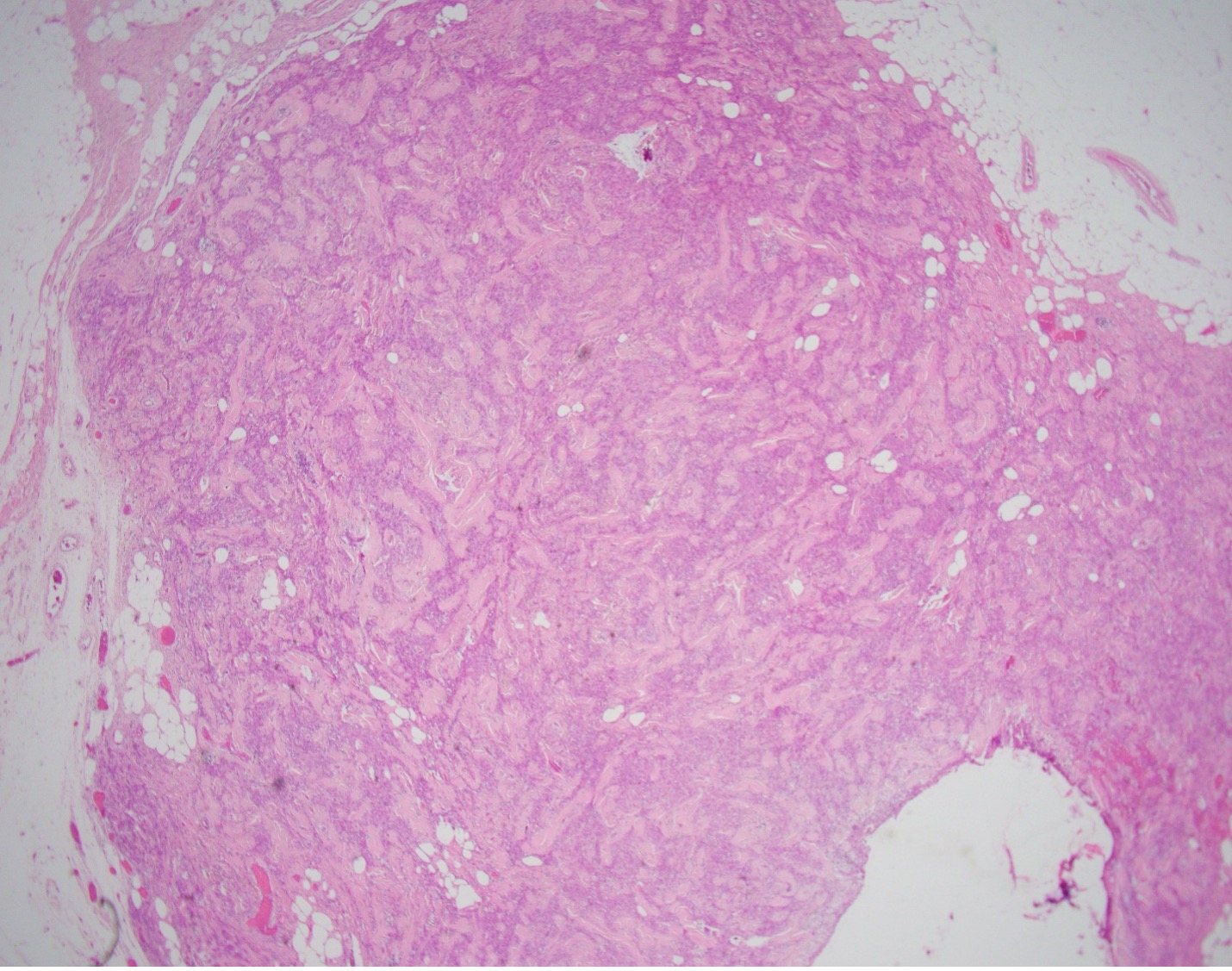
The patient is a 81-year-old male with a palpable breast mass. Imaging demonstrated an oval parallel mass with indistinct margins measuring 14 x 10 x 13 mm in the right breast at 1 o'clock located 1 cm from the nipple. A lumpectomy was performed and representative sections are shown.
What is the best diagnosis?
A. Metaplastic Carcinoma
B. Myofibroblastoma
C. Malignant phyllodes
D. Cellular PASH (Pseudoangiomatous stromal hyperplasia)
Case discussion:
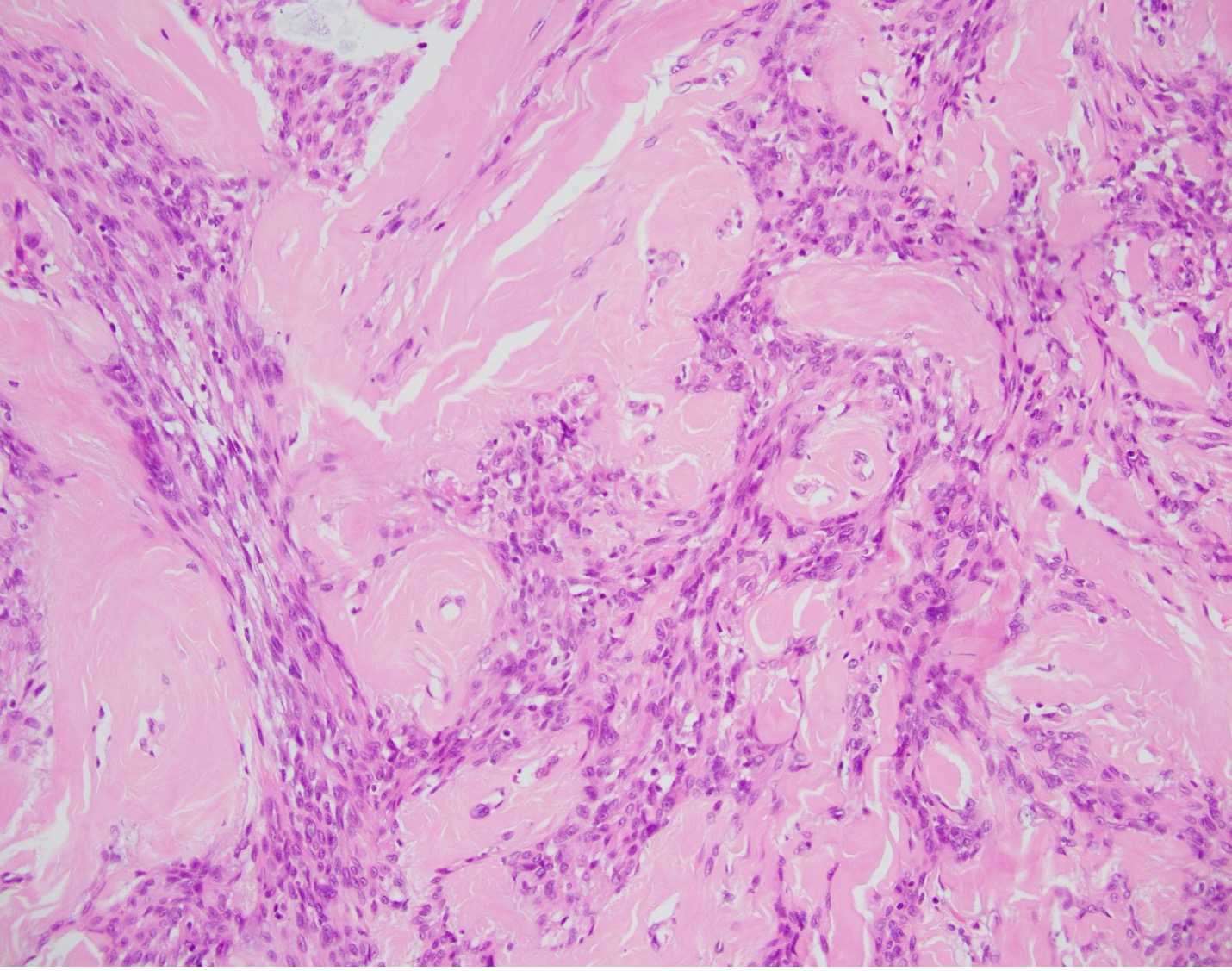
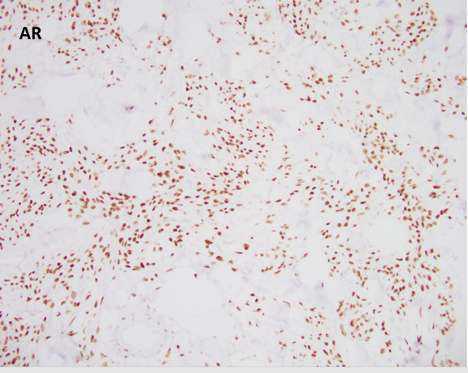
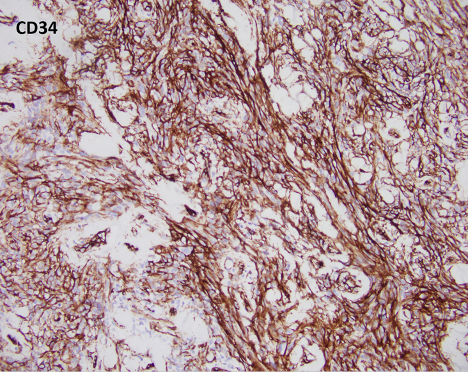
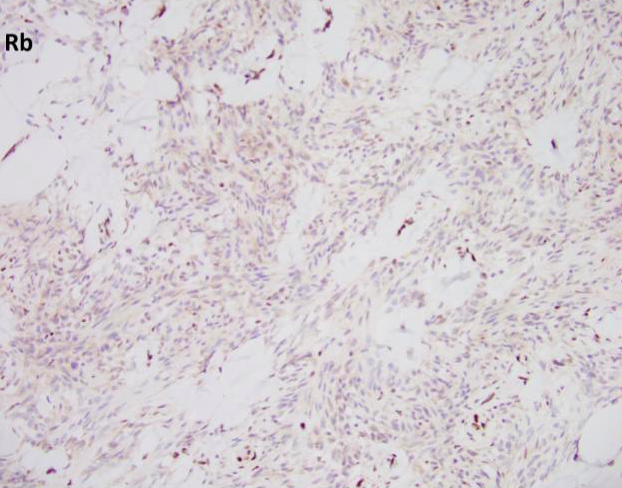
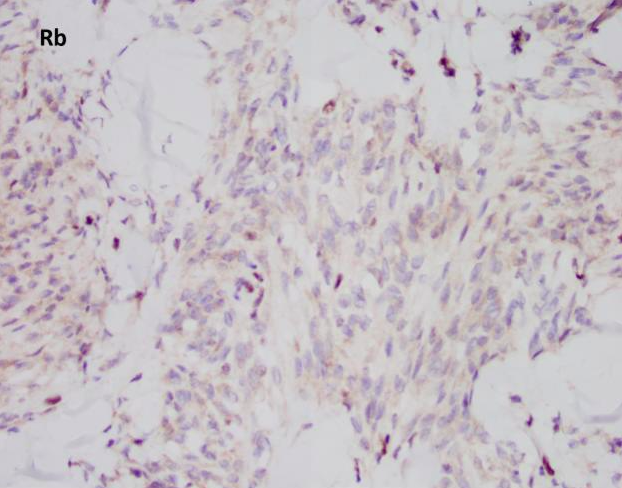
Myofibroblastoma (MFB) is an uncommon myofibroblastic lesion, typically seen in older patients. It occurs in both males and females and usually presents as a slow growing, palpable, painless breast mass. Most lesions are small, 1-4 cm; however, cases of giant myofibroblastomas have been reported. Histologically, the lesion is characterized by a well-circumscribed mass composed of spindle cells intermixed between bundles of hyalanized collagen. Because the neoplasm is myofibroblastic in origin, immunohistochemical markers such as Smooth Muscle Actin (SMA), Muscle Specific Actin (MSA), and Desmin are characteristically positive. Myofibroblastomas are also typically positive for CD34, estrogen receptor (ER), progesterone receptor (PR), and androgen receptor (AR). The cells of interest are negative for cytokeratins. Genetically, the entity is characterized by loss of 13q14 and 16q. As a result, there is inactivation of genes RB1 and FOXO1, and as such, loss of Rb expression via immunohistochemistry. Treatment typically consists of surgical excision with no additional therapy required.
All of the other answer choices may be considered in the differential diagnosis, especially on biopsy. Metaplastic carcinomas can be comprised of spindle cells with or without an epithelioid component. However, the stromal collagen is typically not present and the cytology is much more pleomorphic with frequent mitosis and an infiltrative growth pattern. Additionally, metaplastic carcinomas will be positive for cytokeratin immunohistochemistry and negative for hormone receptors ER/PR/AR, CD34, and desmin/myofibroblastic markers. Phyllodes tumors are also neoplasms of stromal differentiation. Phyllodes tumors, however, show both the presence of spindle cells and benign epithelium, typically creating a “leaf-like” architecture. IHC is positive for CD34 but Rb staining is retained. Pseudoangiomatous stromal hyperplasia (PASH) usually doesn’t form a mass; however, it is a myofibroblastic lesion with a similar staining pattern, SMA, desmin, ER, and PR positive. Histologically PASH has a dense collagenous stroma with prominent slit-like spaces. Additionally, the characteristic genetic alterations found in MFB are not present.
Case contributed by: Xiao Huang, M.D., Ph.D. Assistant Professor, Anatomic Pathology