Case History
Patient with neuroimaging studies showing an 9.0 cm, in greatest dimension, destructive mass arising from dura with osseous extension. Metastatic imaging work up and Pancytokeratin IHC is negative.What would be the top of your differential diagnosis?
A. High grade lymphoma
B. High grade meningioma
C. Squamous cell carcinoma
D. High grade glial neoplasm
Microscopic Description:
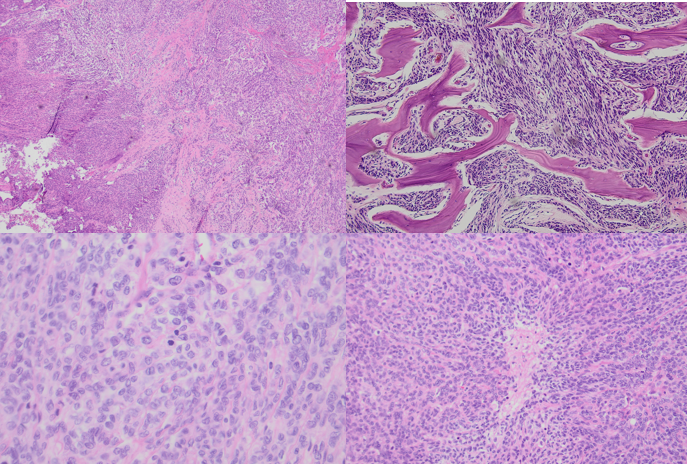
- Microscopic sections show a malignant meningothelial neoplasm with moderately enlarged, irregularly shaped, hyperchromatic nuclei within a background of dense connective tissue. Also present is greater than 20 mitotic figures per high power field, expanded and coalescent fields of spontaneous tumor necrosis, foci of small cell change and frequent prominent nucleoli.
- The malignant meningothelial neoplasm is also infiltrating into marrow spaces of bone.
- Immunohistochemical stains performed are CD45, Pax-5, CD3, CD20, p63, GFAP and pancytokeratin were all negative within the neoplastic cells.
Discussion:
- Anaplastic meningioma is a high grade meningioma with overtly malignant cytomorphology (anaplasia) that can resemble a carcinoma, high grade sarcoma or melanoma
- It has an elevated mitotic count (greater than or equal to 20 mitotic figures per 10 high power field) which defines this as a CNS WHO grade 3 meningothelial neoplasm
- Defined molecular alterations include harboring a TERT promoter mutation and/or having a homozygous CDKN2A and/or CDKN2B deletion.
Reference:
Sahm, F., et al. Meningioma. In: WHO Classification of Tumours Editorial Board. Central nervous system tumours [Internet]. Lyon (France): International Agency for Research on Cancer; 2021 [cited 07/14/2022]. (WHO classification of tumours series, 5th ed.; vol. 6). Available from: https://tumourclassification.iarc.who.int/chapters/45/91.
Case contributed by: Michael Williams, M.D., M.Sc., Neuropathology Fellow, UAB Pathology