Case History
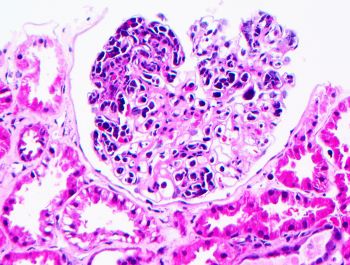
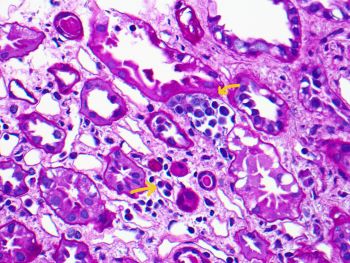
A 51-year-old man presents with AKI and proteinuria. Figures A & B show light microscopy. IF and EM studies are unremarkable.
What is the most appropriate diagnosis?
A. Post-infectious glomerulonephritis
B. Intravascular large B cell lymphoma
C. Cryoglobulinemic glomerulonephritis
D. Extracavitary primary effusion lymphoma
Answer: B. Intravascular large B cell lymphoma (IVLBCL)
Discussion:
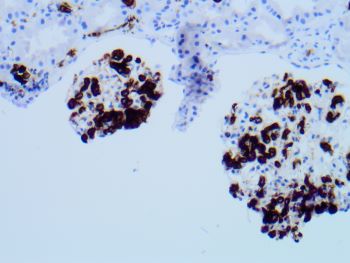
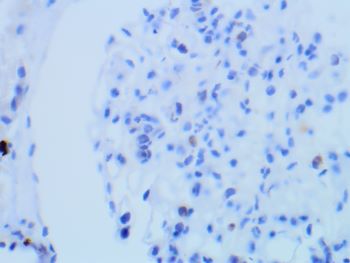
Medium power view of a glomerulus shows near global intracapillary infiltration by large atypical mononuclear cells (endocapillary hypercellularity) without increased mesangial matrix or mesangial hypercellularity ((H&E Fig a). There are no fibrin thrombi or PASH-positive hyaline plugs (pseudo thrombi). No crescent or fibrinoid necrosis is present. Occasional peritubular capillaries (arrows) contain similar intraluminal large atypical mononuclear cells(PASH Fig b). Immunohistochemical stains show diffuse positive staining for CD-20 (Fig c), MUM-1, and BCL-6 and focal positive staining for BCL-2. However, large atypical cells are negative for CD-3 (Fig d), CD10, HHV-8 and EBER. These morphologic features and immunohistochemical staining pattern support the diagnosis of intravascular large B-cell lymphoma (IVLBCL) non-germinal center type, with renal involvement. The absence of immune complex deposits by IF and EM excludes the possibility of immune complex-mediated proliferative glomerulonephritis (GN), mentioned in the choices i.e., post-infectious GN or Cryoglobulinemic GN. Negative HHV8 excludes primary effusion lymphoma.
IVLBCL is a rare subtype of large cell lymphoma, characterized by the proliferation of lymphoma cells within the lumina of small blood vessels, particularly capillaries and post-capillary venules, without an obvious extravascular tumor mass or readily observable circulating lymphoma cells in the peripheral blood. Renal involvement is exceedingly rare; however, when present it typically manifests as renal dysfunction. Most patients diagnosed with IVLBCL are treated with regimens used for diffuse large B cell lymphoma, particularly in combination with Rituximab (anti-CD20 antibody) is the most commonly employed treatment.
Reference:
Arnaud Desclaux, et al. Renal Intravascular Large B-cell Lymphoma: A Case Report and Review of the Literature. (Intern Med 56: 827-833, 2017) (DOI: 10.2169/internalmedicine.56.6406)
Case contributed by: Huma Fatima, M.D., Associate Professor, Anatomic Pathology, Renal Section Head, UAB Pathology