Case History
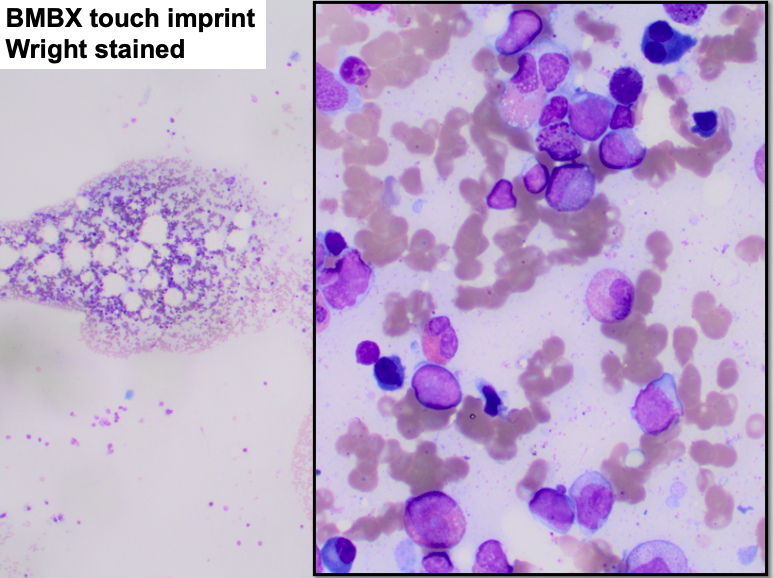
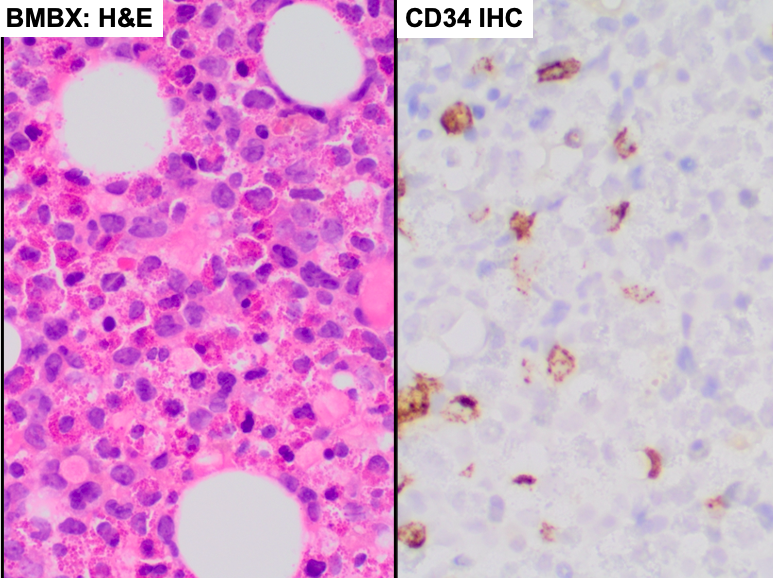
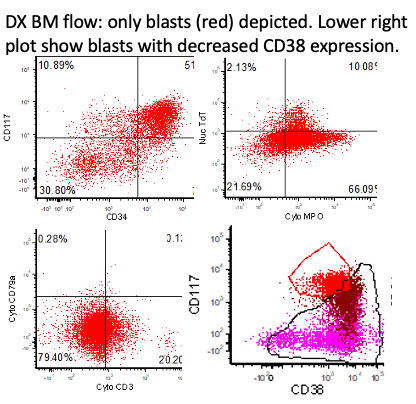
A 33 yo male with pancytopenia (thrombocytopenia >10 years, leukopenia for 3 years), presumed secondary to hypersplenism. Now with neutropenia. This is the first in-house BM assessment. Touch imprint and CD34 IHC of BM bx show 10% blasts with eosinophilia. Flow shows immunophenotypic >20% abnormal myeloblasts.
What is the diagnosis?
A. Myelodysplastic neoplasm with increased blasts 2 (10% blasts)
B. Myelodysplastic/myeloproliferative neoplasm, NOS
C. Acute myeloid leukemia with CBFβ::MYH11 (10% blasts).
D. Myeloid neoplasm associated with germline predisposition
E. Myeloid/lymphoid neoplasms with eosinophilia and defining gene rearrangement.
Discussion:
Correct answer: Acute myeloid leukemia (AML) with CBFβ::MYH11 (10% blasts)
Increased and immunophenotypic abnormal myeloblasts without known reactive causes are diagnostic for a myeloid neoplasm. Although flow shows >20% blasts, morphology with 10% blasts is the gold standard for blast enumeration. While ≥20% myeloblasts are typical of most AML, some myeloid neoplasms with <20% blasts and certain genetic abnormalities behave like AML and are classified as such, as this case.
If FISH studies were negative, then the NGS abnormalities FLT3 and KRAS would favor MDS (answer A) but MDS/NPM (answer B) cannot be excluded and further genetic analysis would be required to rule out answers D and E.
Reference:
https://tumourclassification.iarc.who.int/chapters/63
https://link.springer.com/article/10.1007/s00428-022-03480-8
Case contributed by: John Choi, M.D., Ph.D., Professor, Laboratory Medicine, Director, Flow Cytometry Lab, UAB Pathology