Case History
An 82-year old man with a history of CKD, hypertension and recently diagnosed clear cell carcinoma revealed 2+ proteinuria during preoperative workup for the carcinoma. Non-neoplastic renal parenchyma, following nephrectomy is shown in the figures a & b. Immunofluorescence and electron microscopy studies are unremarkable.
What is the diagnosis?
A. Severe arteriosclerosis
B. Thrombatic microangiopathy (TMA)
C. Atheroembolism
D. Vasculitis
Answer: Athero-embolism OR Cholesterol Crystal Embolism (CCE).
Brief explanation of the answer:
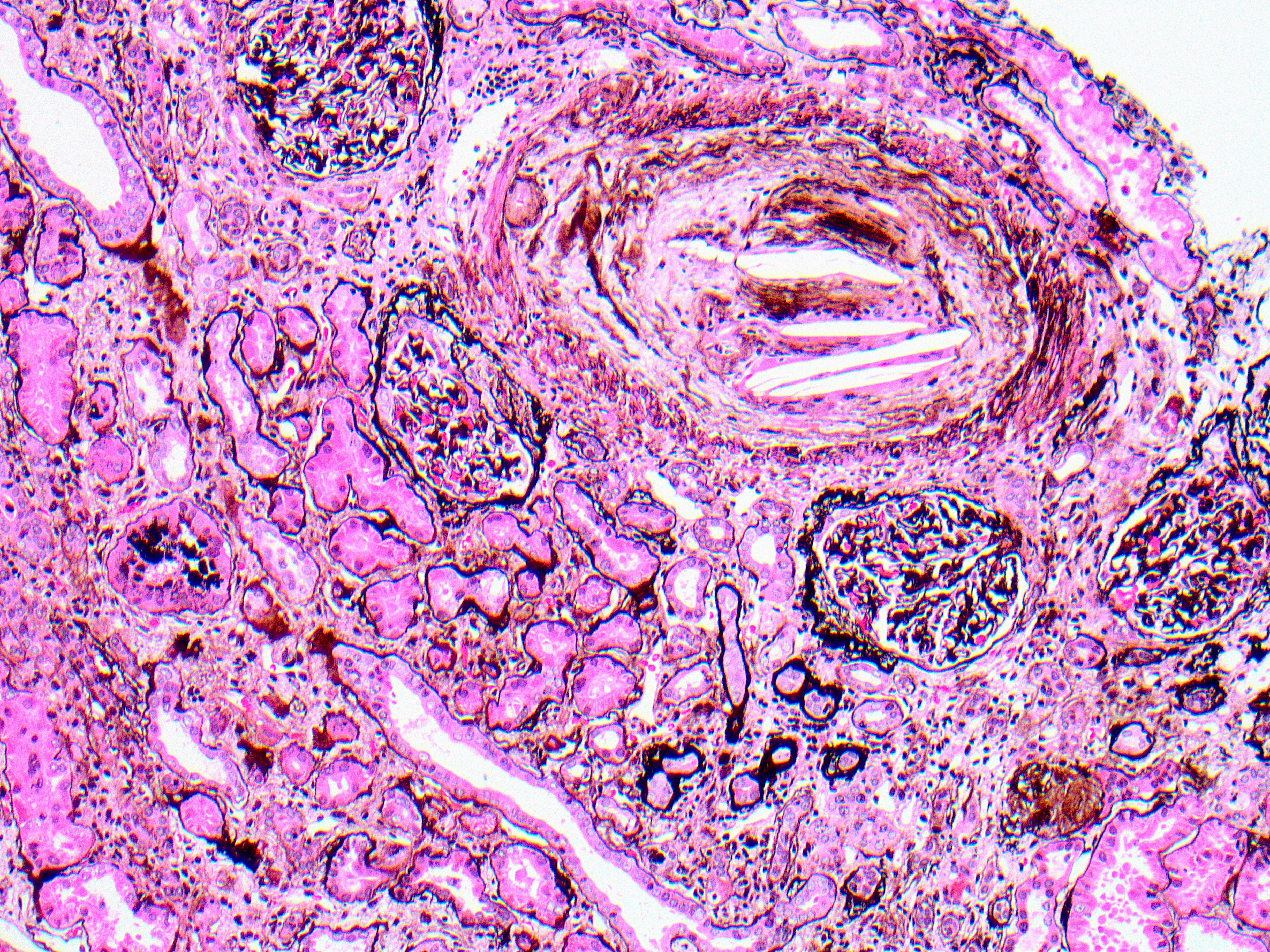
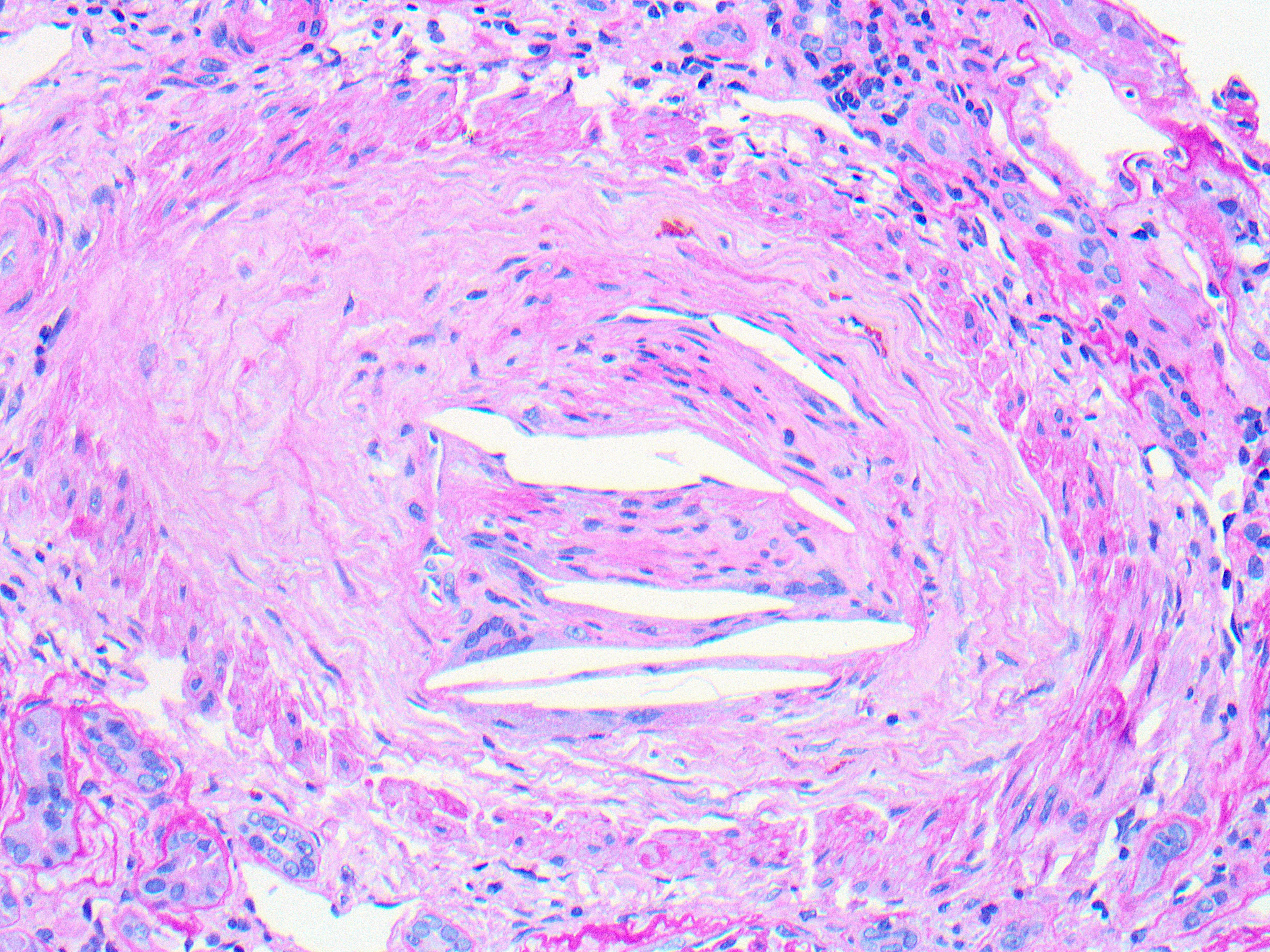
On medium power a cross section of an interlobular artery shows multiple intraluminal cleft-shaped spaces, reflecting the empty spaces left after the dissolution of cholesterol by standard processing (Jones silver Fig a). Chronic ischemic glomerular and tubulointerstitial injury is also evident by focal periglomerular fibrosis and tubulointerstitial scarring, respectively. High power of the same artery shows intimal fibrosis and mild cellular proliferation with occasional mononuclear cells and multinucleated giant cells (arrow) surrounding cleft-like spaces, representing a dissolved cholesterol embolus (PASH Fig b).
Atheroembolic renal disease, also known as cholesterol crystal embolism (CCE), occurs in older patients who have underlying severe atherosclerosis. Cholesterol emboli usually occur following invasive procedures or vascular surgery; however, it may occur spontaneously. The kidney is the most commonly involved organ, although any organ can be involved. Patients present with acute renal failure, hypertension, livedo reticularis, leg pain, gastrointestinal symptoms and vision loss. A subset of CCE may present as chronic, stable, and asymptomatic renal insufficiency like in this case. This is likely due to frequent and slow crystal migration from ruptured atherosclerotic lesions. There is no specific therapy available at present. Patients with acute kidney injury may require heparin-free dialysis to avoid further embolization. Prognosis in general is poor.
Case contributed by: Huma Fatima, M.D., Associate Professor, Anatomic Pathology, Renal Section Head, UAB Pathology