Case History
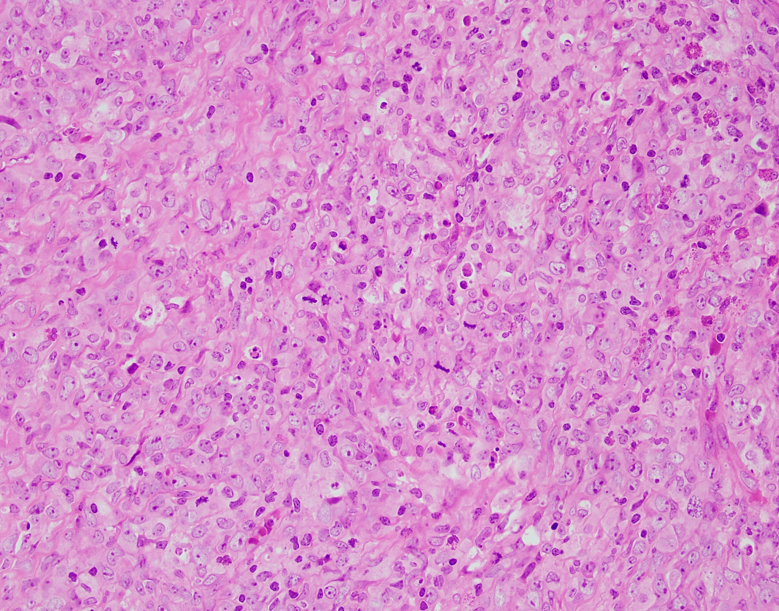
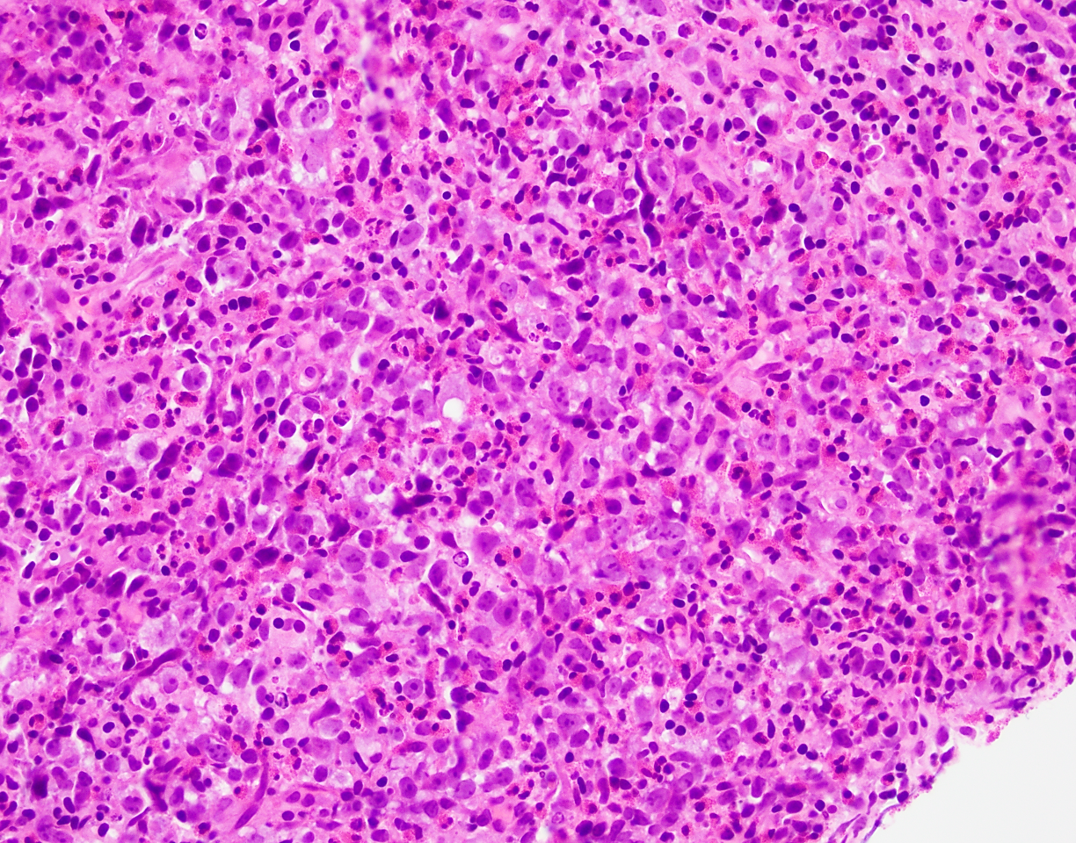
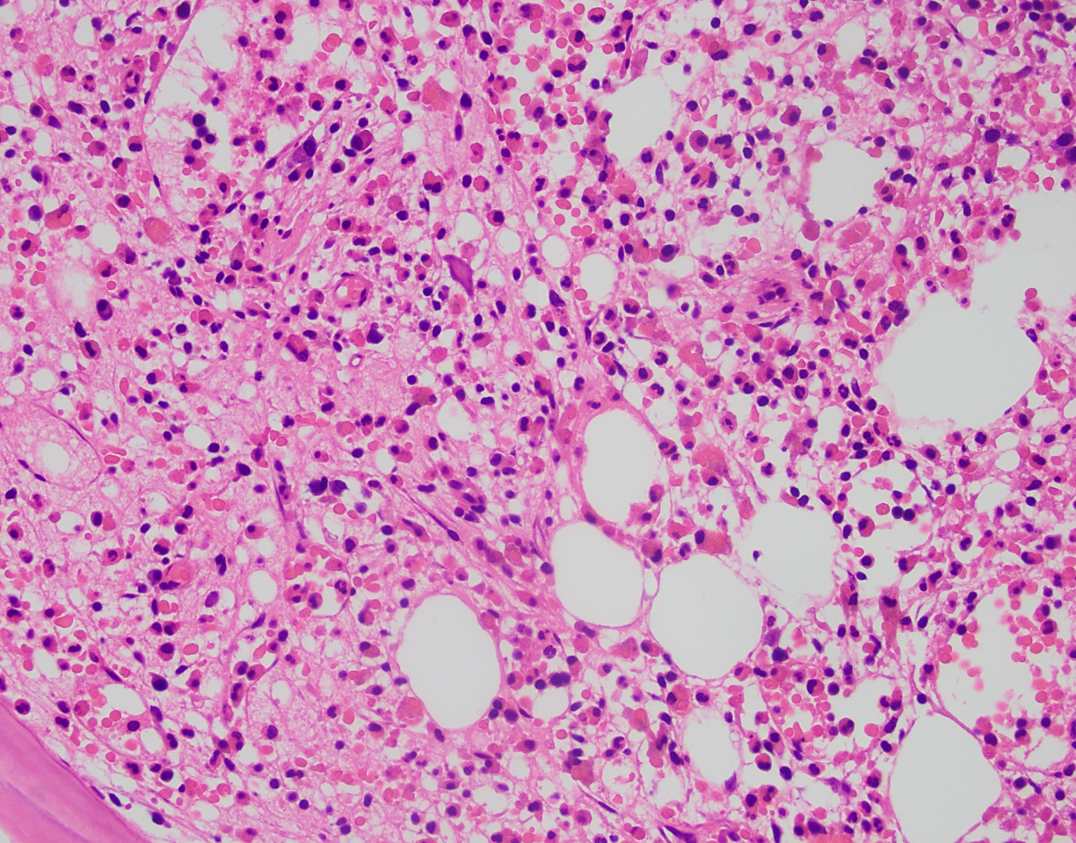
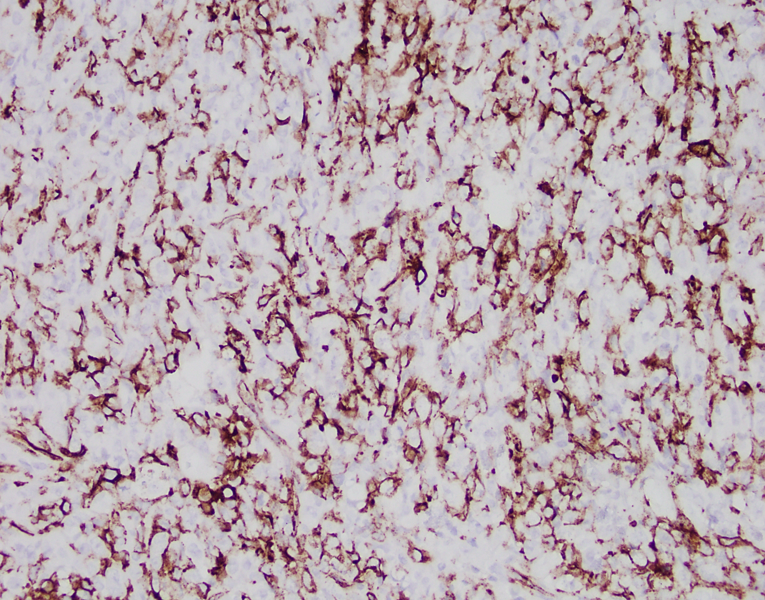
60 yr old male with a mandibular mass and lymphadenopathy. CBC showed marked absolute eosinophilia (60%; 6.06 x 10^3/cm). The mass is CD34+, CD45+, CD33+, patchy + for CD43, MPO. A) mandibular mass, B) submandibular lymph node, C) CD34, D) bone marrow bx
What is the diagnosis?
A. Blastic plasmacytoid dendritic cell neoplasm
B. Myeloid sarcoma with eosinophilia and tyrosine kinase gene fusion
C. Histiocytic sarcoma
D. Langerhans cell sarcoma
Answer: B. Myeloid sarcoma with eosinophilia and tyrosine kinase gene fusion
Discussion:
Sections of the mandibular mass and submandibular lymph node show markedly large, atypical cells with prominent nucleoli, with brisk mitotic activity. Eosinophils are prominent in the lymph node. The peripheral blood shows relative and absolute eosinophilia (60%; 6.06 x 10^3/cm), and the bone marrow biopsy showed eosinophilia with clusters of mast cells but no increase in myeloblasts.
Myeloid sarcomas have variable staining patterns, but markers typically positive are lysozyme, CD43, CD33, and MPO. CD34 can be positive (30-40% overall) in immature myeloid sarcomas. CD34 is strongly positive in this case, which is certainly helpful in distinguishing from other blastic or high-grade neoplasms like BPCDN.
Given the presence of myeloid sarcoma and profound eosinophilia in the blood, marrow, and lymph nodes, we had a suspicion for a tyrosine kinase gene fusion. In the new ICC, this case falls into the category of “Myeloid neoplasm with eosinophilia and tyrosine kinase gene fusion.” The genes include PDGFRA, PDGFRB, FGFR1, JAK2, with the newly-added FLT3 and ETV6::ABL1. The WHO classification is similar.
FISH performed on the submandibular lymph node biopsy show that 82% of the cells have the FIP1L1::PDGFRA gene fusion due to an interstitial deletion in the 4q12 region; and FISH on the bone marrow aspirate also showed that 15% of the cells have the FIP1L1::PDGFRA gene fusion due to an interstitial deletion in the 4q12 region.
The FIP1L1::PDGFRA gene fusion confirmed the diagnosis. This specific fusion is due to a “cryptic” deletion in the 4q12 region. This gene fusion can be detected by nested RT-PCR, a break-apart probe, a probe for the CHIC2 gene, or a 4q12 Tri-color Rearrangement Probe set consisting of three differently colored probes all located in the FIP1L1-PDGFRA region of chromosome 4 band q12. The typical presentation with the PDGFRA gene fusion is a chronic eosinophilic leukemia-like picture, although our case showed myeloid sarcoma. The PDGFRA/B cases show excellent responses to TKIs.
Case contributed by: Taylor Pickens, M.D., Hematopathology Fellow, UAB Pathology