Case History
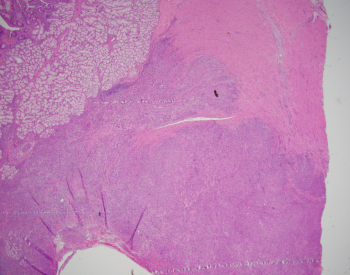
A 32-year-old male presents with abdominal pain and bloating. He undergoes a distal subtotal gastrectomy for a 6 cm ulcerated mass located in the pylorus.
How is this tumor best classified?
A. Gastric (adeno) carcinoma with lymphoid stroma
B. Hepatoid adenocarcinoma
C. Undifferentiated adenocarcinoma
D. Poorly cohesive carcinoma
Answer: A. Gastric (adeno)carcinoma with lymphoid stroma
Discussion:
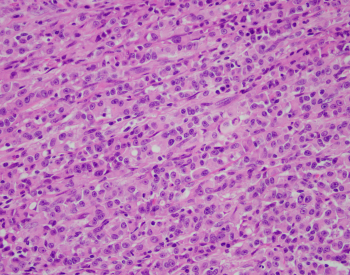
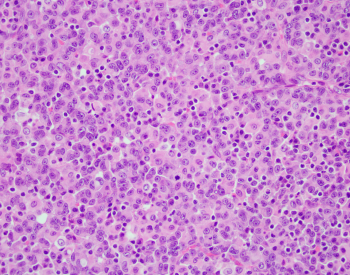
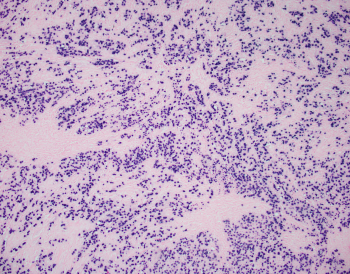
Gastric (adeno)carcinoma with lymphoid stroma has been reported to account for 1-7% of all gastric cancers, and has also been known as lymphoepithelioma-like carcinoma and medullary carcinoma. This subtype normally has a poorly differentiated morphology characterized by irregular sheets, trabeculae, ill-defined tubules, or syncytia of polygonal cells embedded within a prominent lymphocytic infiltrate with intraepithelial lymphocytes. The tumor are most often seen in the proximal stomach (unlike this patient) and are most commonly seen in males. Reported rates of EBV infection in this subtype vary from 22.5-100% with EBER in situ hybridization used for virus detection. A subset of gastric carcinomas with MSI and/or mismatch repair deficiency has a similar histologic phenotype with a different molecular profile. EBV-associated gastric carcinomas tend to lack TP53 mutations, have prevalent ARID1A and PIK3CA mutations, and may have amplification of JAK2 and PDL1. EBV-associated gastric carcinomas tend to have better overall survival compared to conventional gastric carcinoma counterparts thanks to targeted therapies.
Case contributed by: Christine Pesoli, M.D., GI Pathology Fellow, UAB Pathology