Case History
A 59-year-old female with a history of ESRD attributed to hypertension, a renal transplant in 2004 on maintenance immunosuppression. Admission for E. coli sepsis with severe AKI a month prior; now with uremic symptoms, creatinine 6.0 mg/dL (baseline 1.9), normal renal ultrasound. Allograft biopsy shown.
Treatment options include:
A. Chemotherapy
B. Antimicrobial therapy
C. Increase immunosuppression
D. Plasmapheresis
Discussion
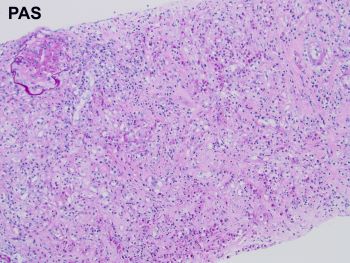
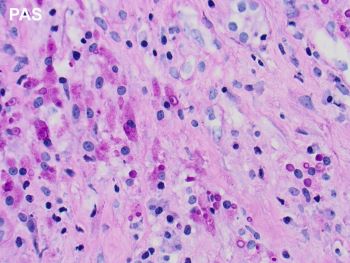
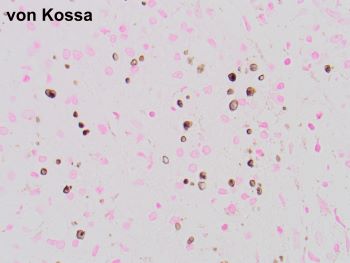
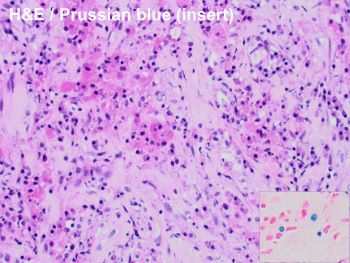
The images of the biopsy show the characteristic features of malakoplakia with obliteration of the renal cortex by a diffuse interstitial inflammatory infiltrate mainly composed of histiocytes with granular eosinophilic cytoplasm. Many of these histiocytes contain targetoid structures positive for PAS, calcium and iron diagnostic of Michaelis Gutman bodies. These represent laminated mineralized concretions that result from the deposition of calcium in phagolysosomes overloaded with breakdown products of bacteria.
Malakoplakia (which means “soft plaque” based on the clinical appearance), is a rare inflammatory disorder that most commonly affects the genitourinary system of women. When affecting the kidney, it is associated with a history of urinary tract infections, most frequently Escherichia coli. The pathogenesis of the disease is thought to be due to a defect in the phagocytic function with incomplete clearance of bacterial organisms in patients with disorders of the immune system, or immunosuppressed states. The latter includes solid transplant patients, such as in this case, where the malakoplakia may compromise allograft function and could result in graft loss. Early diagnosis and prompt start of treatment are essential.
Although there are no guidelines or standard criteria for management, treatment modalities in the setting of renal transplantation include antimicrobial therapy (correct answer B), surgical or radiological debulking and reduced immunosuppression. Successful outcomes have been reported with a combination approach of use of antibiotics with intracellular activity along with immunosuppression reduction. Plasmapheresis is a treatment option for patients with antibody mediated rejection, increased immunosuppression is contraindicated in these patients, and chemotherapy may be used in the treatment of malignant neoplasms, which malakoplakia can mimic clinically and radiologically.
References:
Graves AL, Texler M, Manning L, Kulkarni H. Successful treatment of renal allograft and bladder malakoplakia with minimization of immunosuppression and prolonged antibiotic therapy. Nephrology (Carlton). 2014 Apr;19 Suppl 1:18-21. doi: 10.1111/nep.12194. PMID: 24460630.
Honsova E, Lodererova A, Slatinska J, Boucek P. Cured malakoplakia of the renal allograft followed by long-term good function: a case report. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012 Jun;156(2):180-2. doi: 10.5507/bp.2012.020. PMID: 22660224.
Kinsella PM, Smibert OC, Whitlam JB, Steven M, Masia R, Gandhi RG, Kotton CN, Holmes NE. Successful use of azithromycin for Escherichia coli-associated renal allograft malakoplakia: a report of two cases. Eur J Clin Microbiol Infect Dis. 2021 Dec;40(12):2627-2631. doi: 10.1007/s10096-021-04270-x. Epub 2021 May 14. PMID: 33990891.
Case contributed by: Andrea Kahn, M.D., Professor, Anatomic Pathology, GYN Section Head, UAB Pathology