Case History
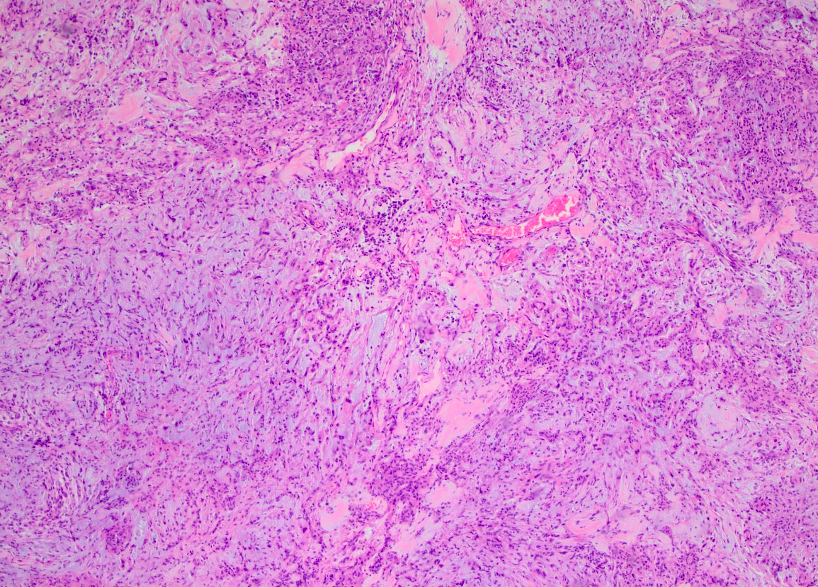
A 60-year-old male presented with a slowly enlarging, contrast-enhancing left lateral ventricular mass.
What is the best diagnosis?
A. Choroid plexus papilloma
B. Choroid memingioma
C. Intracranial mesenchymal tumour, FET::CREB fusion-positive
D. Rhabdoid meningioma
Answer: C. Intracranial mesenchymal tumor, FET::CREB fusion-positive
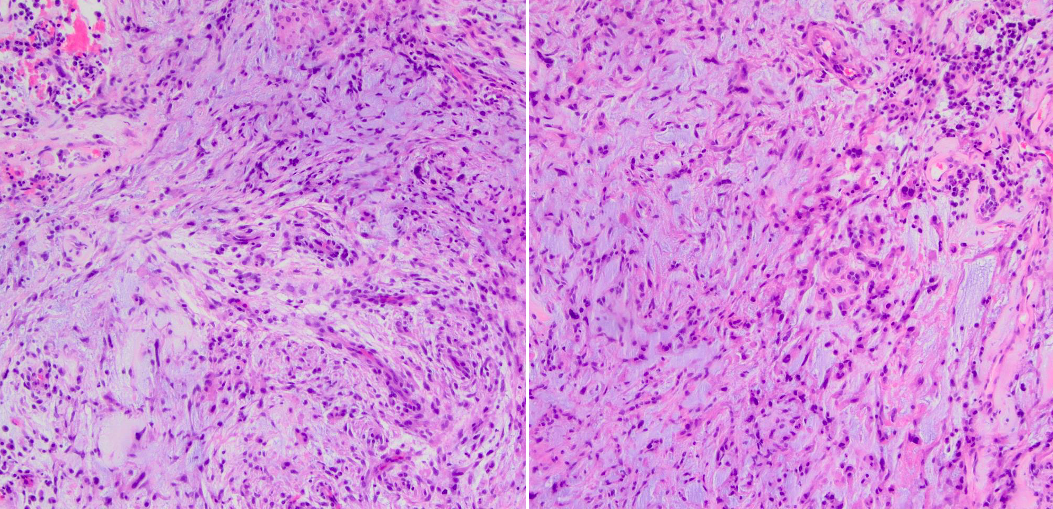
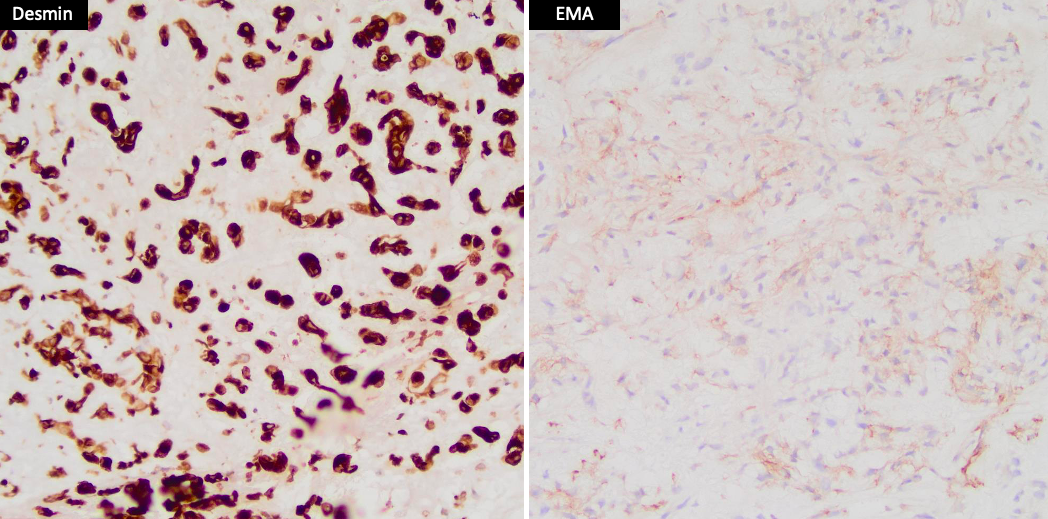
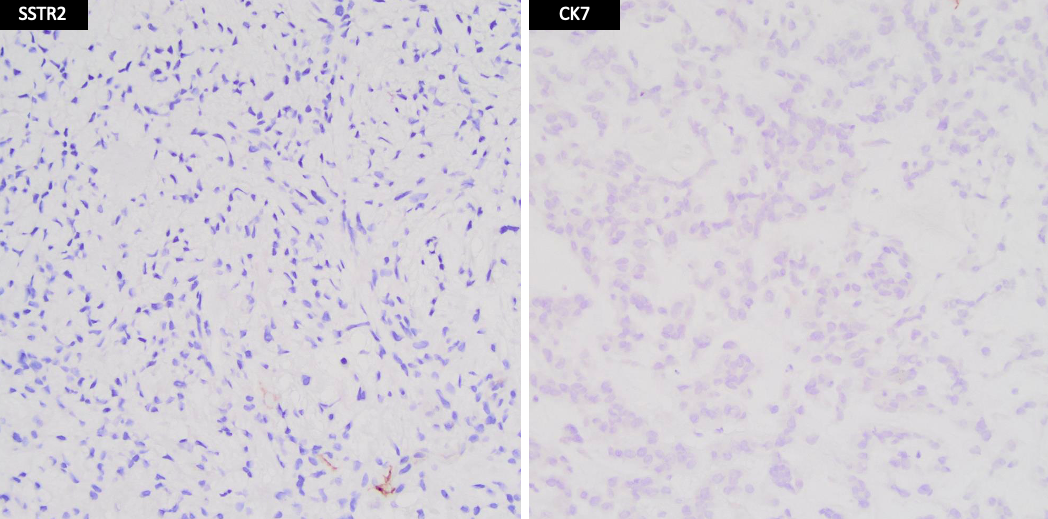
Intracranial mesenchymal tumors with FET::CREB fusion originate intracranially and exhibit variable histomorphology. They are characterized by the fusion of FET RNA-binding protein family gene (usually EWSR1, rarely FUS) with a CREB family transcription factor (CREB1, ATF1, or CREM). The histomorphology ranges from syncytial or sheet-like growth to reticular cord-like structures. Tumor cell morphology varies from epithelioid/rhabdoid cells to stellate/spindle cells to monotonous round cells. Some tumors contain fibrous septa that separate nodules of tumor cells. Myxoid stroma is characteristic, but not all examples exhibit it. The immunohistochemical profile varies, with EMA, CD99, and desmin commonly showing positive results. Negative markers include SSTR2A, OLIG2, GFAP, CAM5.2, myogenin, MYOD1, myoglobin, SMA, MSA, melan-A, HMB45, MITF, nuclear STAT6, and CD34. SMARCB1 and SMARCA4 expression is retained, while the Ki-67 labeling index is generally low. The full spectrum of clinical behavior is not yet known, but it ranges from slow growth to rapid recurrences.
Case contributed by: Rati Chkheidze, M.D., Assistant Professor, Neuropathology, UAB Pathology