Case History
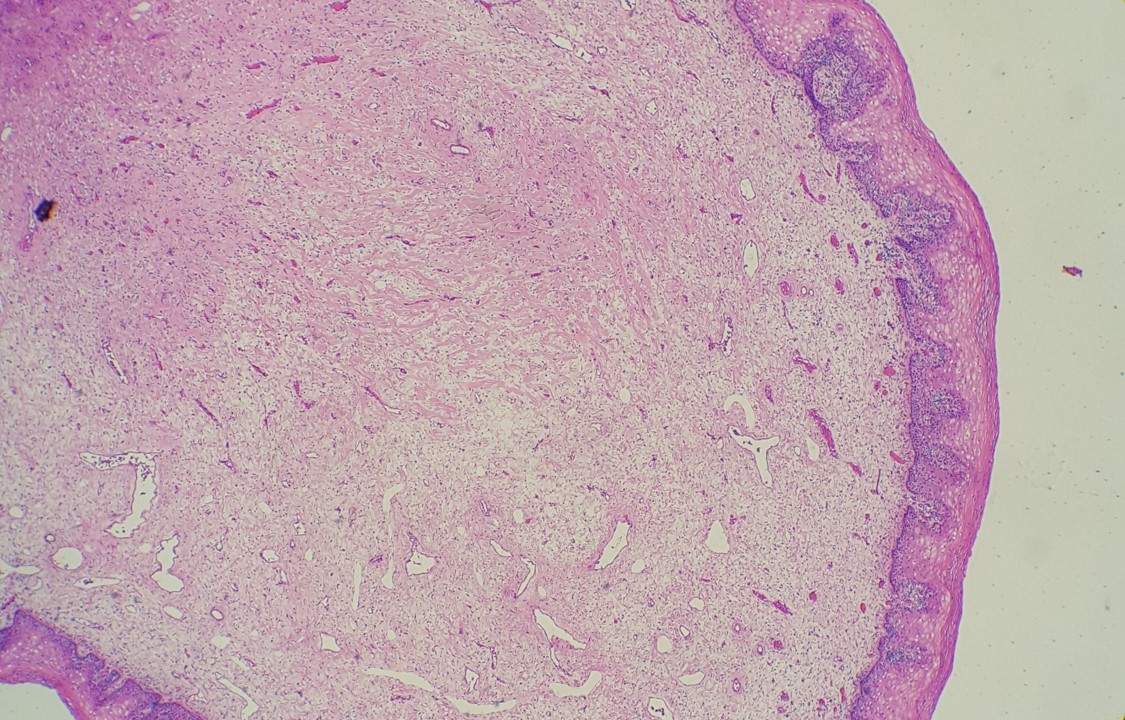
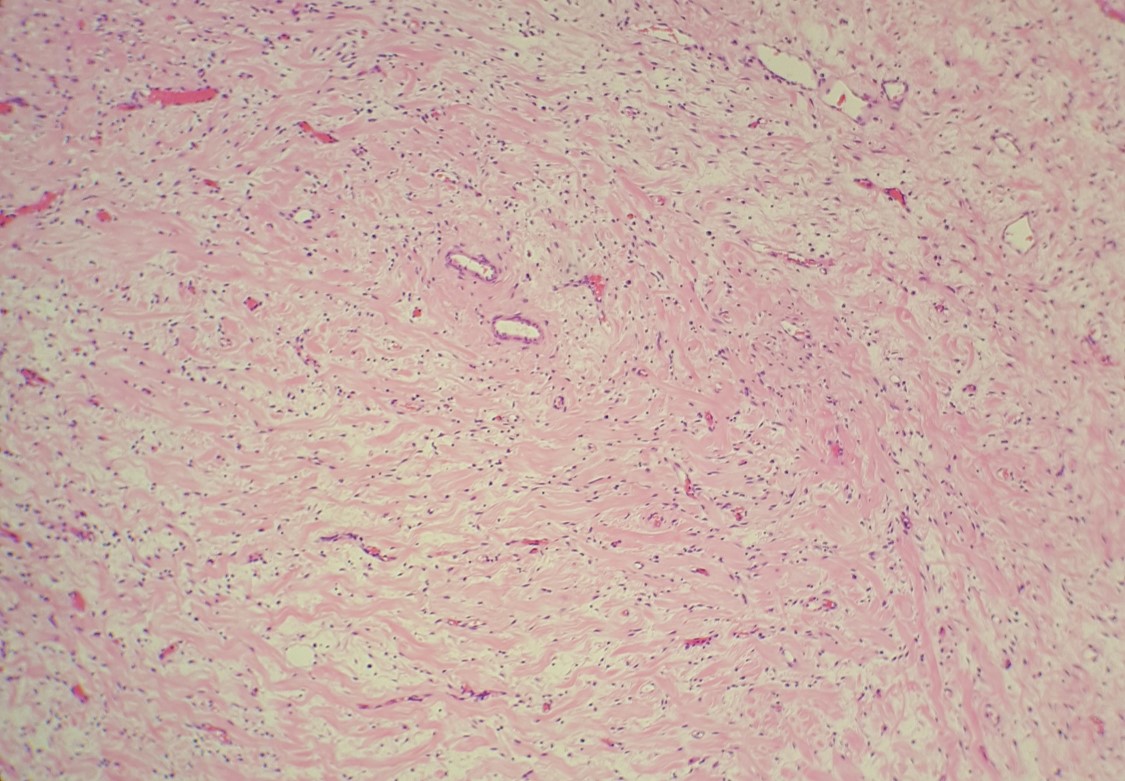
A 58-year-old-female with a persistent gastric ulcer presented to ER with acute abdominal pain and underwent total gastrectomy. During surgery, an enlarged lymph node was sent to frozen analysis and it was reported to be reactive. Grossly, a 2.7 x 2.5 cm perforated ulcer was noted on posterior gastric wall. The entire lesion was submitted for microscopic examination.
What is your diagnosis of this case?
- A. Perforated gastric adenocarcinoma
- B. Perforated gastric lymphoma
- C. Perforated stomach due to Sarcina Ventriculi
- D. Perforated stomach due to Staph aureus
Answer:
C, “Perforated stomach due to Sarcina Ventriculi”
Discussion:
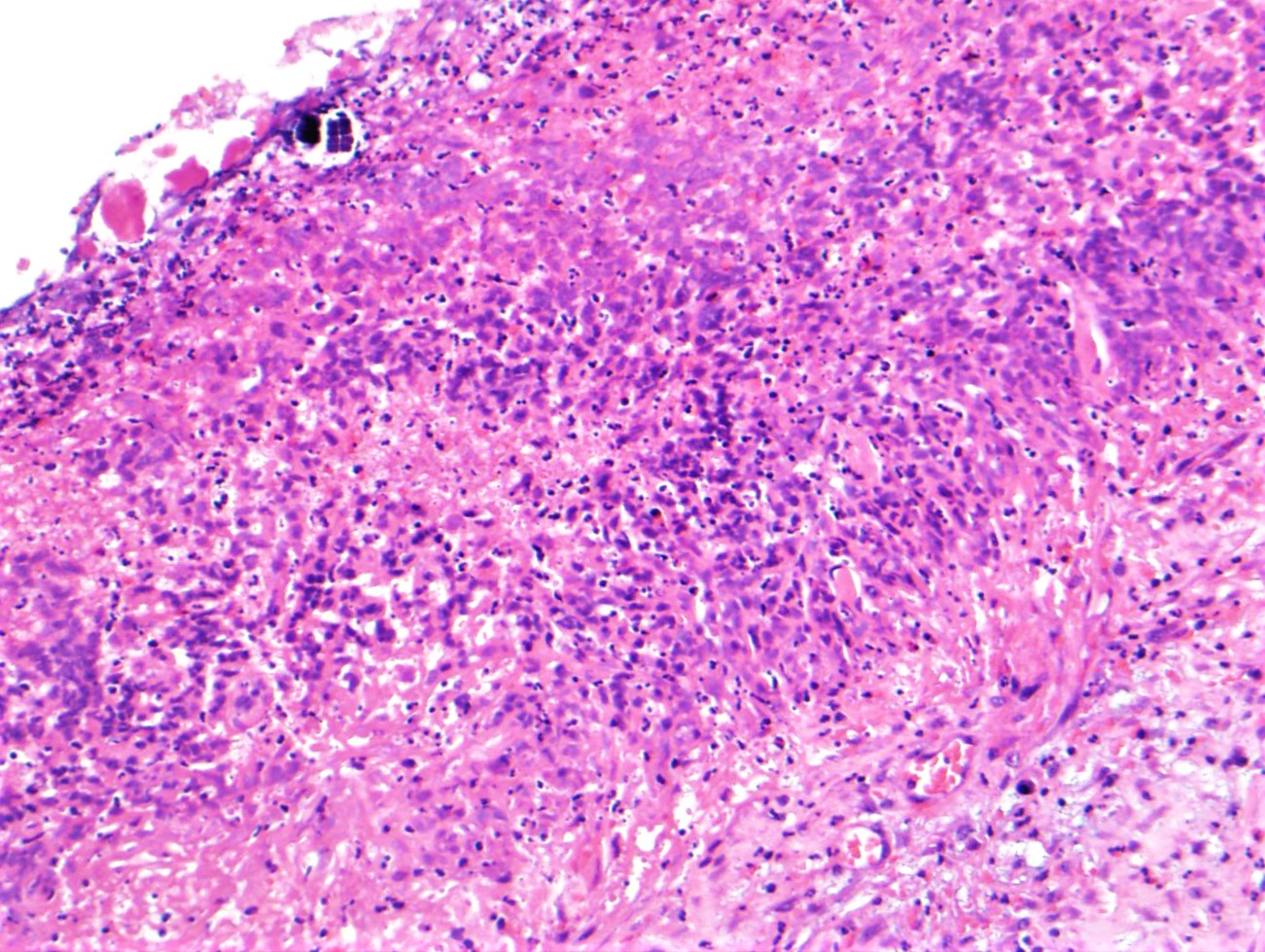
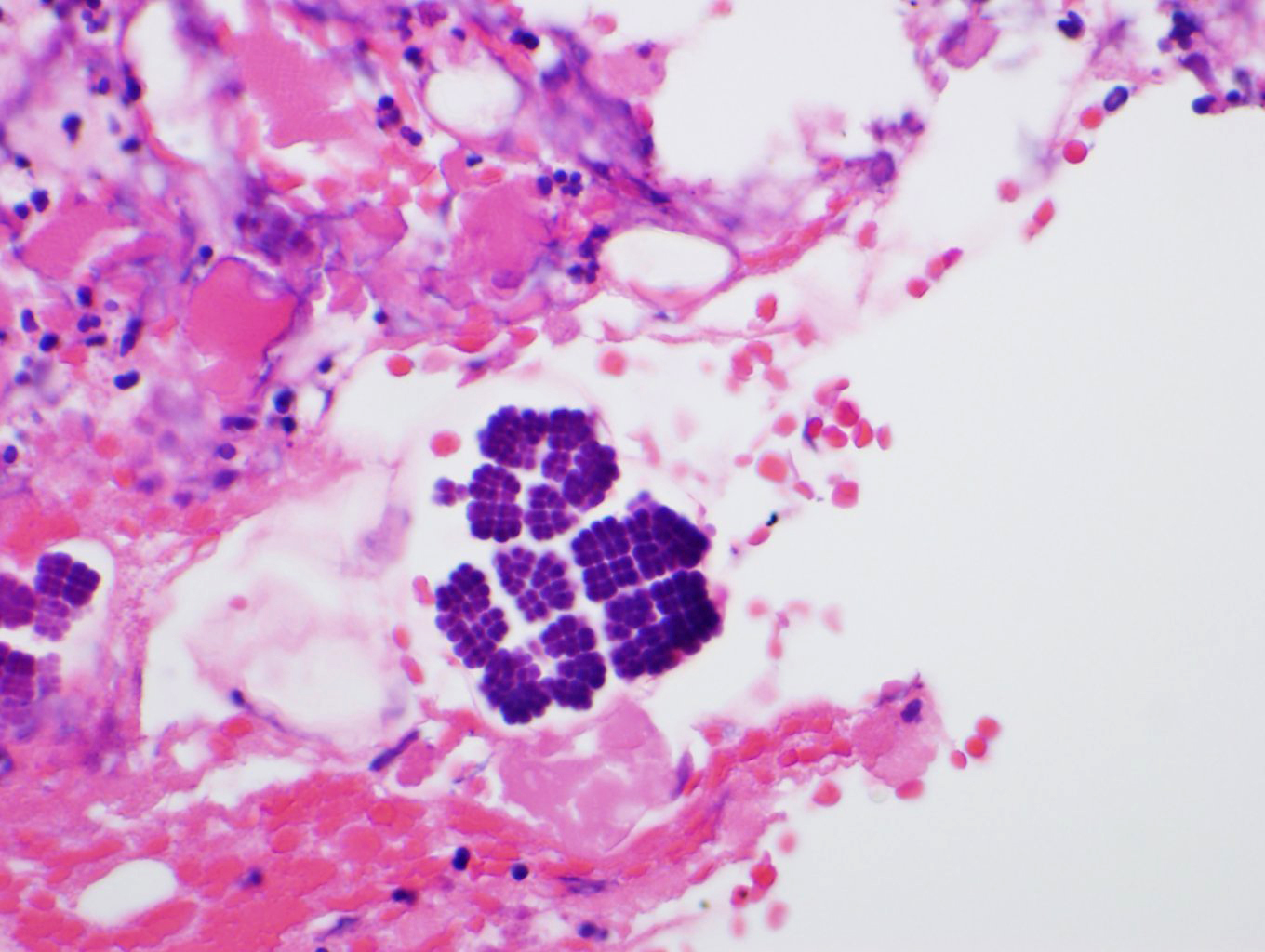
The entire ulcer was submitted for microscopic examination. No malignancy or H. Pylori identified. However, multiple bacterial cocci were noted at the ulcer bed. They are basophilic-stained and cuboid-shaped bacteria that arranged in tetrad packets, consistent with Sarcina ventriculi.
Sarcina ventriculi is anaerobic gram-positive coccus that grows in an acidic environment. It is typically diagnosed with a hematoxylin-eosin stain and, if needed, with a Gram special stain. It was first described by Goodsir in 1842 as a human pathogen. The pathogenic status of Sarcina in human is still unclear. However, association of Sarcina with a patient with gastric perforation, emphysematous gastritis, and peritonitis as well as occurring in the background of gastric adenocarcinomas has been reported. It can normally be found in the soil and air, where it can survive for years by forming spores at alkaline pH. It ferments Carbohydrate as an energy source. Sarcina species, whose natural habitat is the soil, is probably ingested with soil particles present in the food. Various reports in veterinary literature have implicated the Sarcina species in the development of gastric dilatation and death in livestock, cats and horses.
Differential diagnoses for S ventriculi are Sarcina maxima and Staphylococcus species. The most helpful feature in light microscopy to differentiate S ventriculi from S maxima is the thick extracellular layer present on the outer surface.
It is important to recognize this bacterium in gastric biopsies, particularly of patients with delayed gastric emptying, because they respond to treatment. Current reports indicate successful eradication of the organism, with treatment usually consisting of metronidazole in combination with another antibiotic and/or a gastrointestinal agent.
References:
Ratuapli SK, Lam-Himlin DM, Heigh RI. Sarcina ventriculi of the stomach: a case report. World J Gastroenterol. 2013;19(14):2282-5. doi: 10.3748/wjg.v19.i14.2282. Review. PubMed PMID: 23599657; PubMed Central PMCID: PMC3627895.
Al Rasheed MR, Senseng CG. Sarcina ventriculi : Review of the Literature. Arch Pathol Lab Med. 2016 Dec;140(12):1441-1445. Review. PubMed PMID: 27922772.
Alvin M, Al Jalbout N Emphysematous gastritis secondary to Sarcina ventriculi. Case Reports 2018;2018:bcr-2018-224233.
Case contributed by: Sameer Al Diffalha, M.D., Assistant Professor, Anatomic Pathology