Case History
A mid 60’s-year-old male with metastatic prostate cancer presents with dysphagia and chest pain. An upper gastrointestinal endoscopy reveals few superficial esophageal ulcers, 27 to 32 cm. The biopsy findings shows in the Figure A (H & E, 20) and Figure B (high magnification, x40) and Figure C (polarizing microscopy). What is your diagnosis?
- Inadequate specimen
- Fungal esophagitis
- Pill esophagitis
- Foreign body
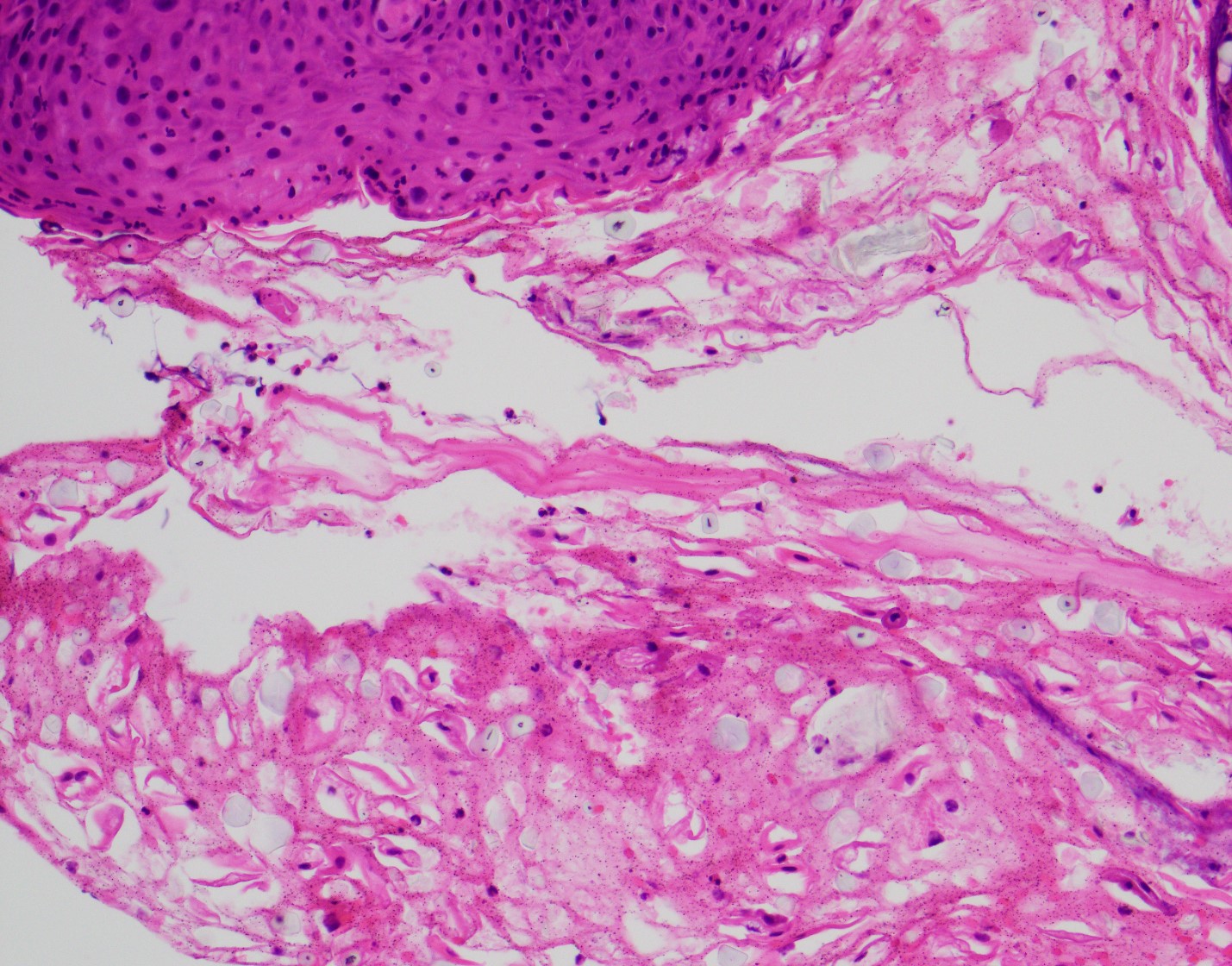 Fig. A: Endoscopic biopsy (H&E Stain, X20)
Fig. A: Endoscopic biopsy (H&E Stain, X20) 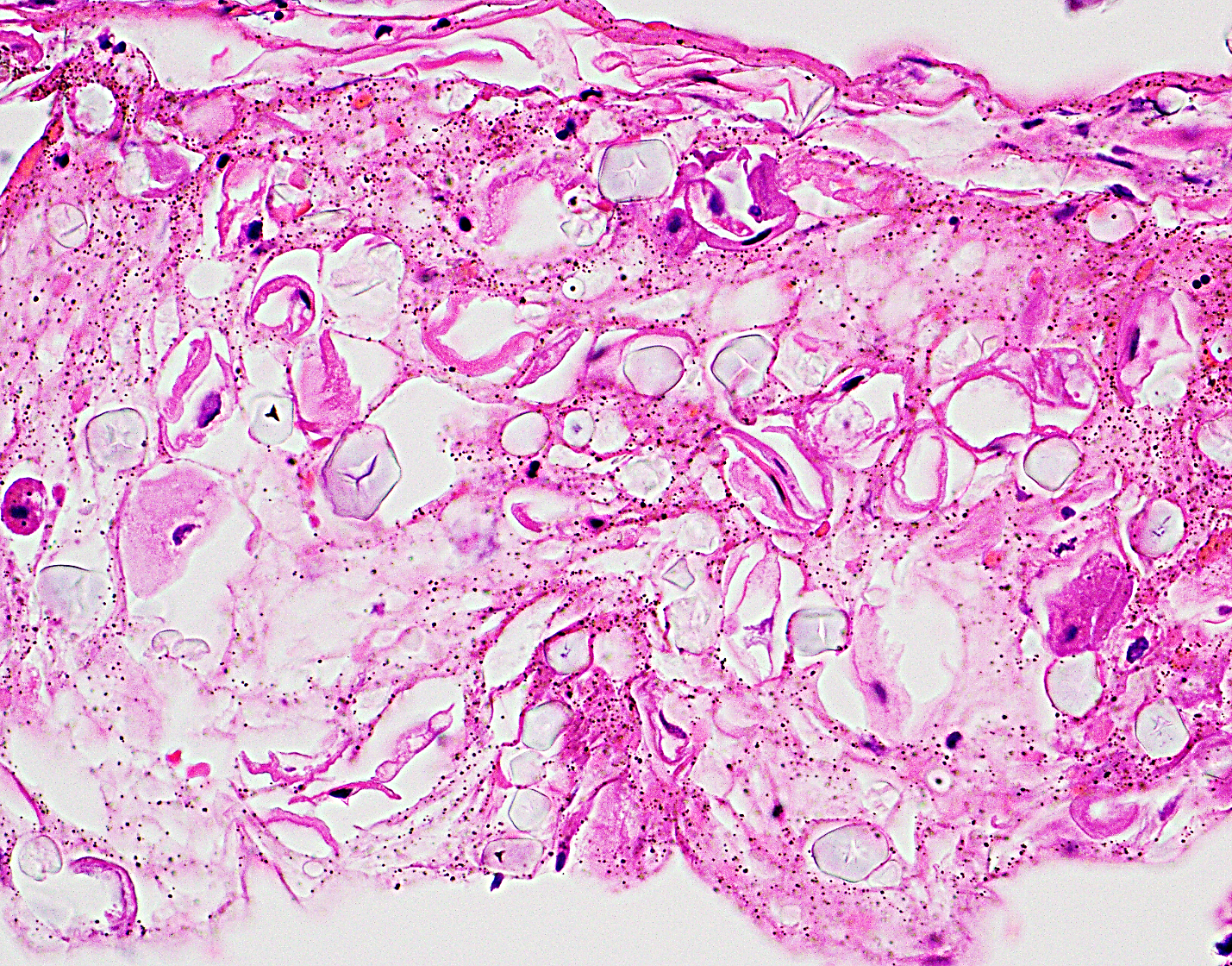 Fig. B High magnification (x40)
Fig. B High magnification (x40) 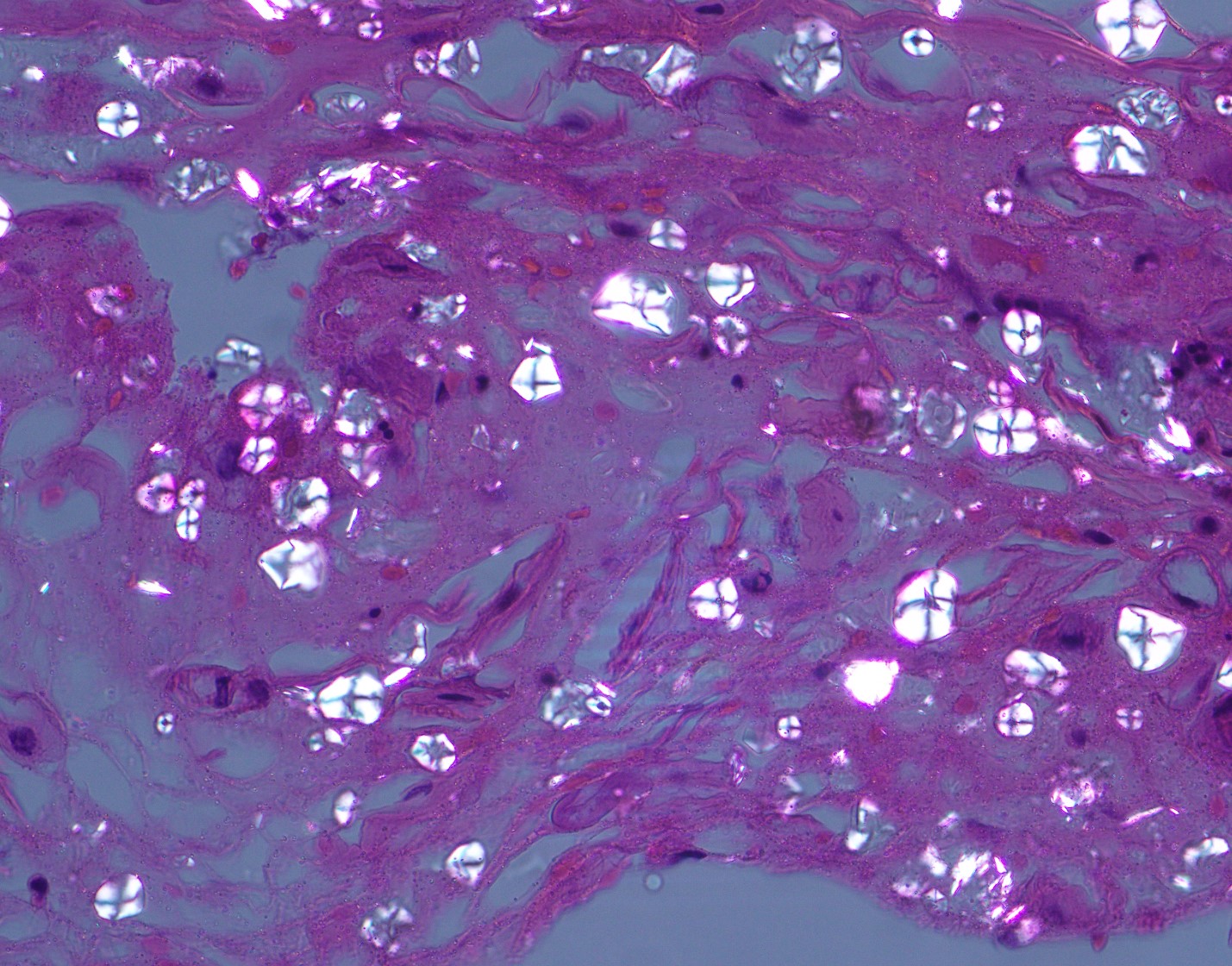 Fig. C: Findings under polarized light
Fig. C: Findings under polarized light Answer: E:) Foreign body- Starch granules with “Maltese cross” birefringent pattern.
In Figure 1 (H & E stain), multiple blue/shiny small, variably shaped structures are present with detached, degenerated squamous cells. Adjacent squamous epithelium contains superficial neutrophilic infiltrate (upper left), suggestive of active esophagitis. GMS stain and immunostains for CMV and HSV 1/2 are all negative (the results not shown). Further evaluation using polarized light showed the “Maltese cross” pattern (Figure 2).
Starch powder applies to surgical gloves and may cause a granulomatous reaction with associated prior procedure. Accidental contamination during specimen handling may occur as well. Microscopically small, refractile, bluish/glassy spherical or spore-like structures are observed and subsequent examination with polarized light shows “Maltese cross” birefringent pattern.
Differential diagnosis includes pill fragments (antibiotics, biphosphonate, NSAIDS, iron), fungal elements (Candida) or other foreign bodies (Talc, food debris).
Pill or drug-induced esophagitis is usually associated with direct mucosal injury. Causative agents include potassium chloride, NSAIDs, antibiotics, iron, and bisphosphonate. Biopsies show esophagitis with inflammatory exudate and erosion/ulcers. Polarizable crystalline material may be seen (e.g., alendronate: yellow crystals).
Candida esophagitis is the most common fungal infection of the esophagus. Fungal forms, yeast and pseudohyphae within fibirinopurulent debris and/or invading squamous epithelium are main features.
Talc (hydrated magnesium silicate) is found in cases with operative sites, pleurodesis, and IV drug users. Talc particles are birefringent under polarized light and induces a granulomatous reaction.
Esophagitis is caused by a variety of physical, chemical, infectious agents, and secondary involvement to systemic diseases. Since the patient in this case has been suffering from multiple medical conditions and taking a large number of drugs as well, it is very difficult to specify single causative agent of the esophagitis. A lesson to learn from this case- Polarized light microscopy- highly recommended in patients with esophagitis if there is a history of drugs, prior procedures, or foreign body/crystalline material is seen on a routine microscopic examination.
References:
Jadhav KB, Gupta N, Ahmed MB. Maltese cross: Starch artifact in oral cytology, divulged through polarized microscopy. J Cytol. 2010 Jan;27(1):40-1.
Pinto LS, da Silva AA, León JE, Jorge J. Letter to the editor: starch artifacts in oral biopsy specimen. Med Oral Patol Oral Cir Bucal. 2008 Jun 1;13(6):E336-7
Maguire A, Sheahan K. Pathology of oesophagitis. Histopathology. 2012 May;60(6):864-79
Grin A, Streutker CJ. Esophagitis: old histologic concepts and new thoughts. Arch Pathol Lab Med. 2015 Jun;139(6):723-9