Case History
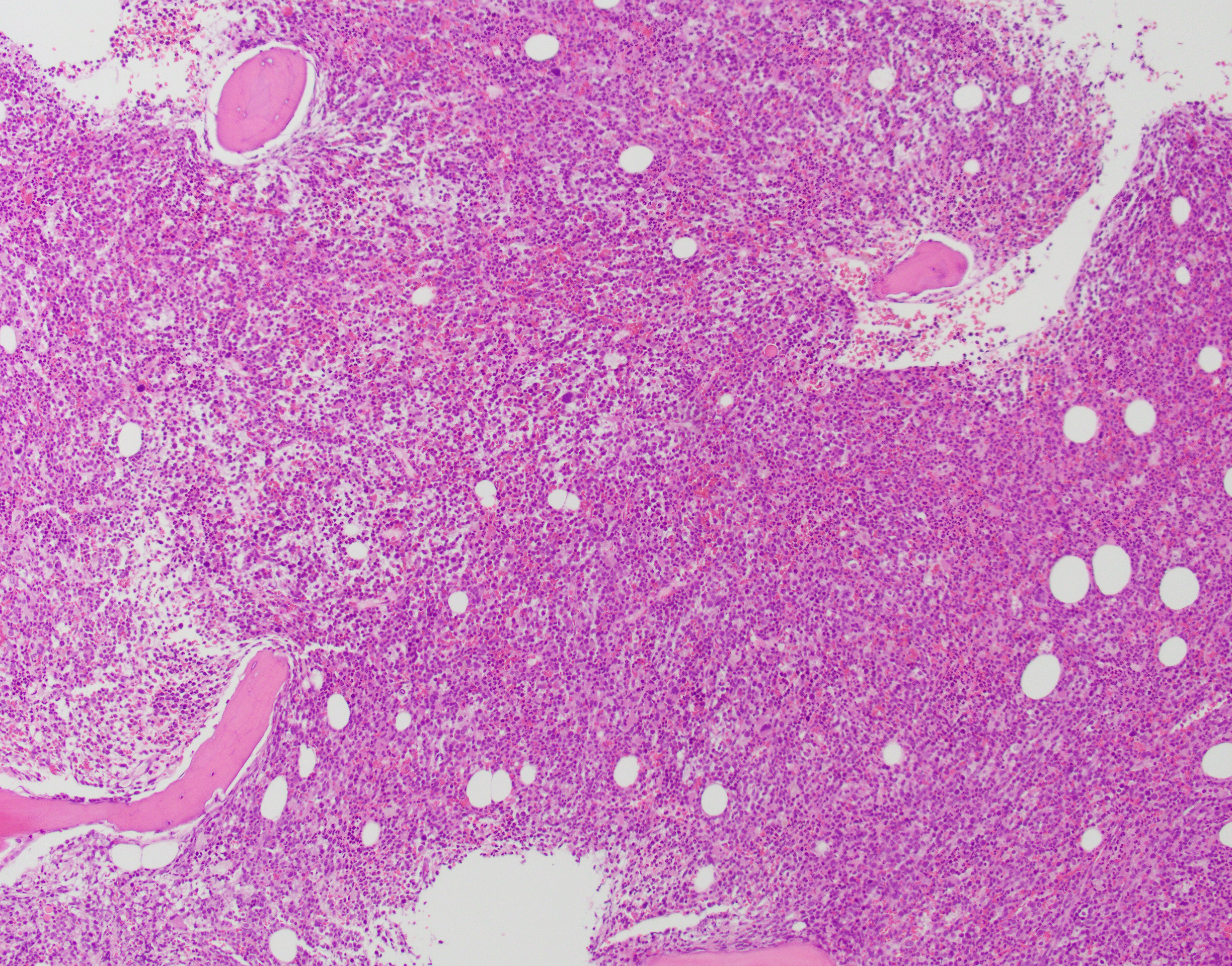
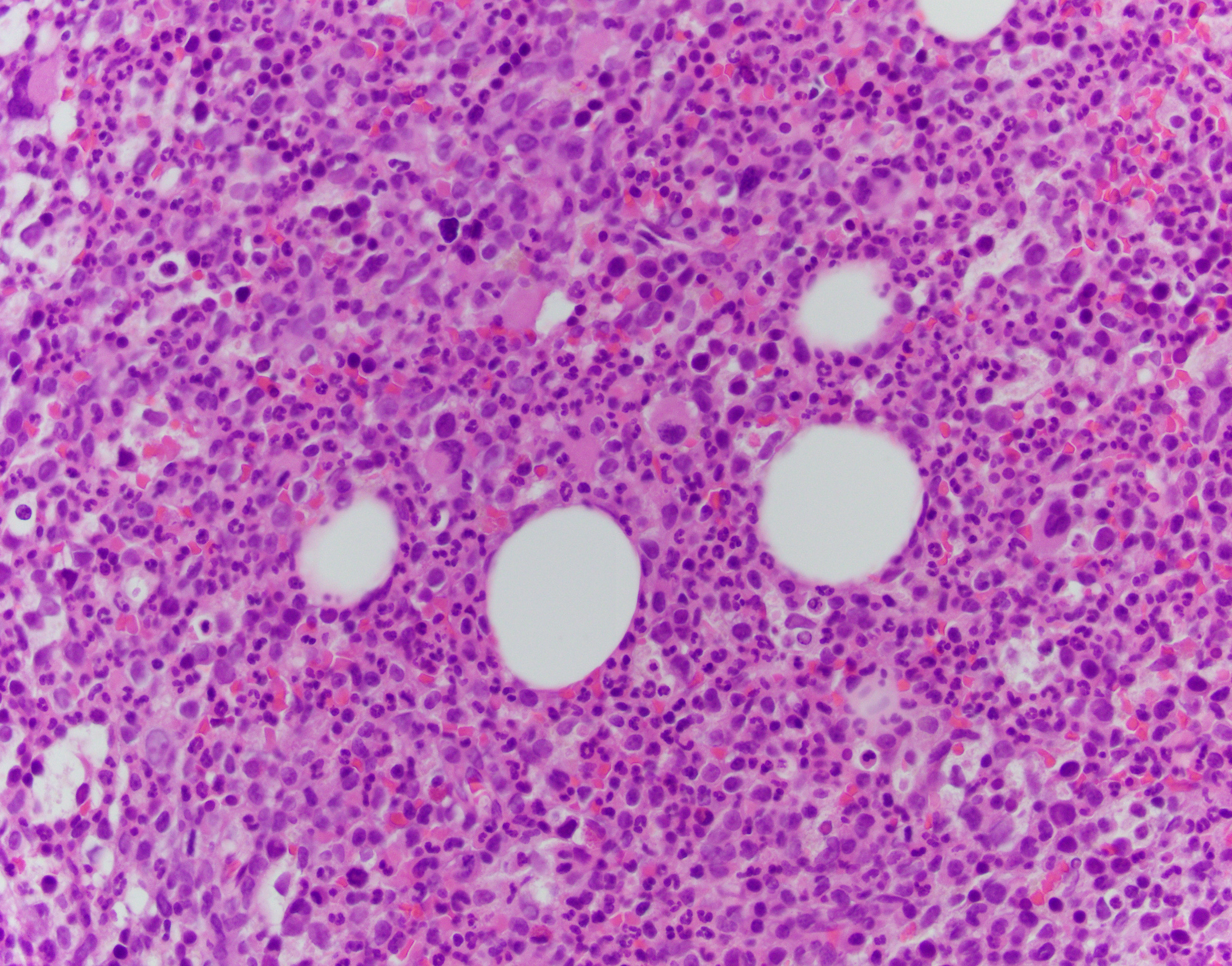
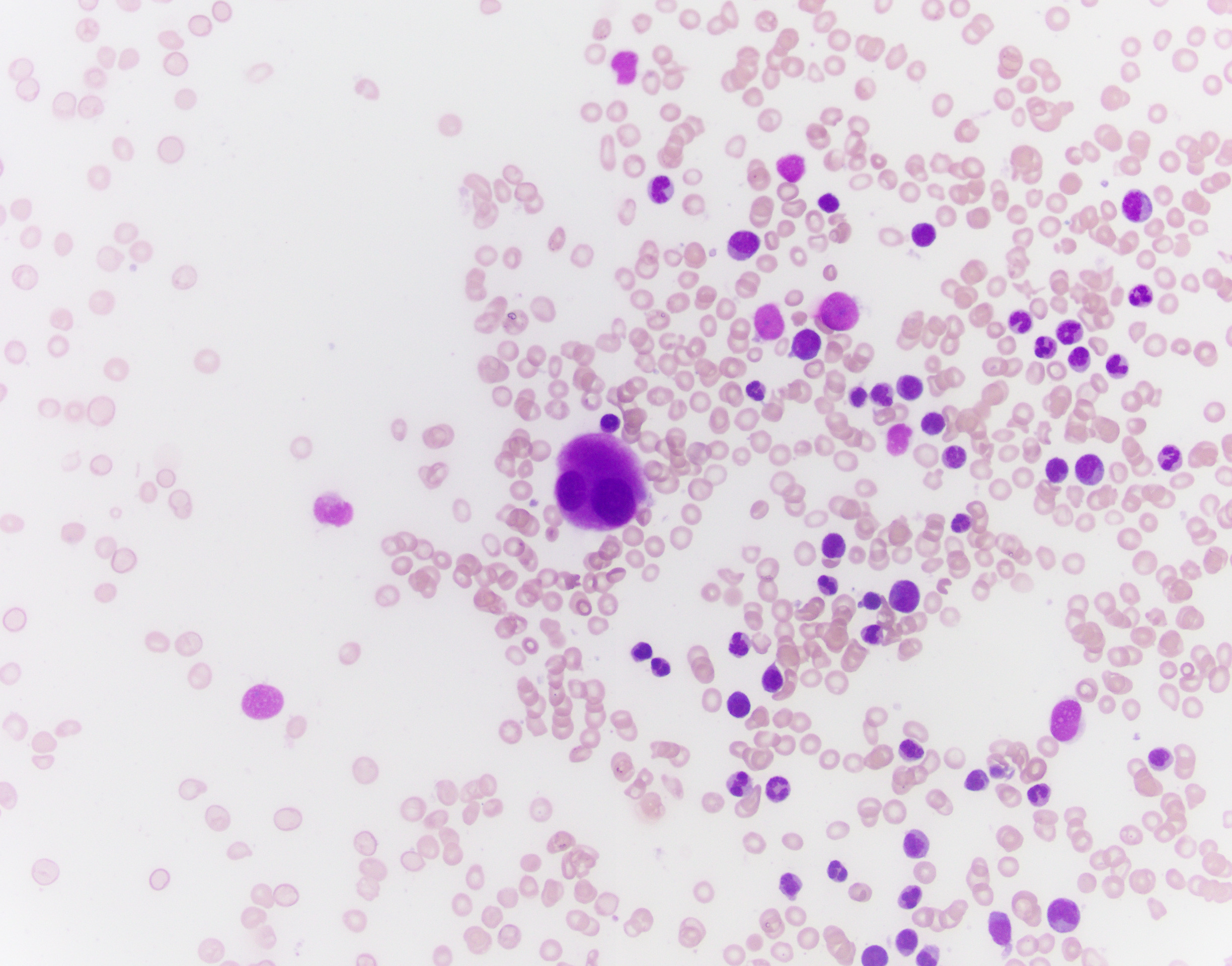
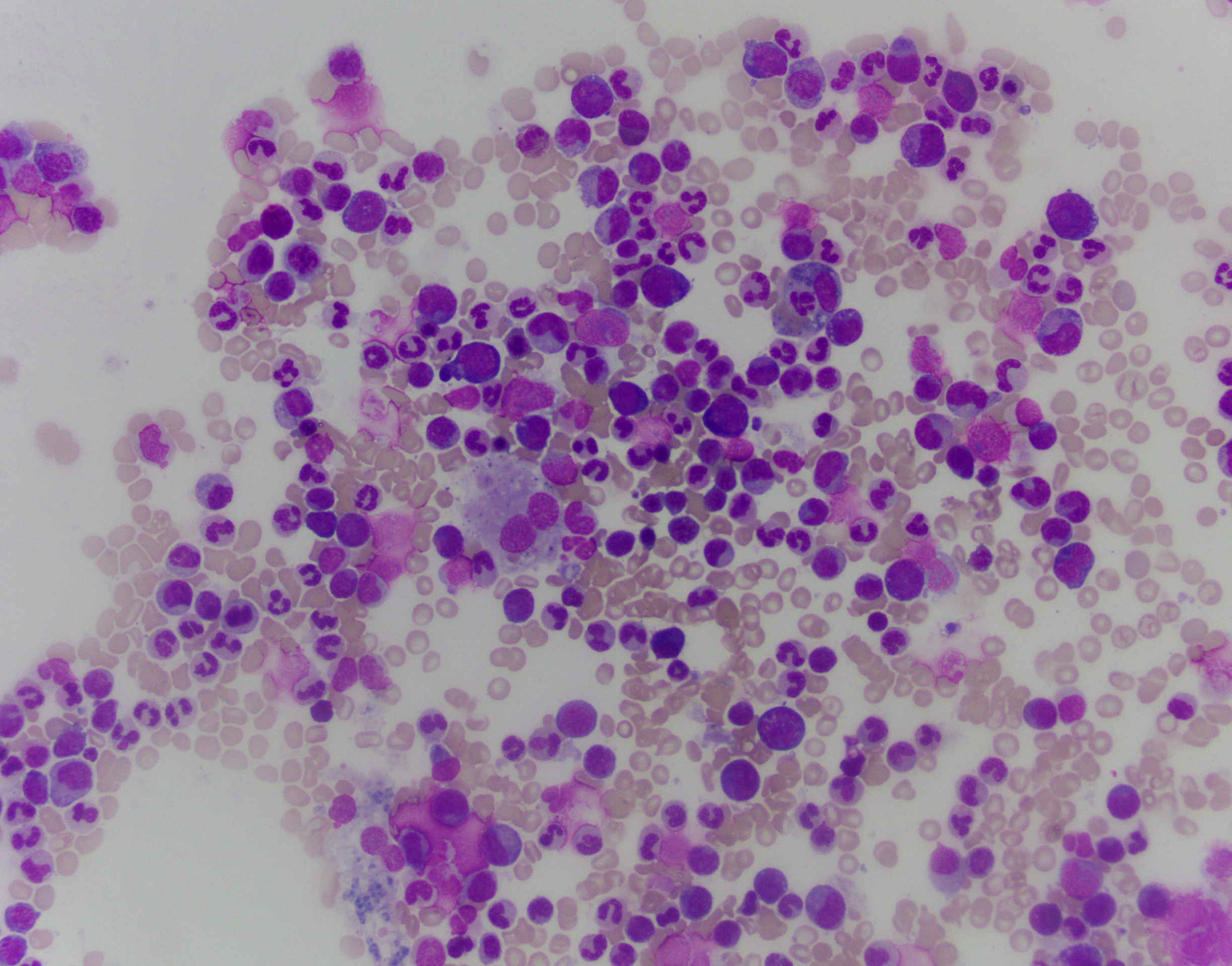
The patient is a 76-year-old male with anemia (Hgb 8.6) and thrombocytopenia (15,000/microliter). Of note, serum copper levels are low. Photomicrographs of the bone marrow aspirate and biopsy are provided.
What is the most appropriate top diagnostic line?
- Dysplasia, see comment
- AML-MRC
- MDS-EB1
- MDS-NOS
Correct answer: A. Dysplasia
The patient's bone marrow biopsy shows a hypercellular marrow with dysmegakaryopoiesis and no overt increase in blasts on routine stains. In a patient with cytopenias and this morphology, the diagnosis is unfortunately rarely straightforward. The differential diagnosis of entities that can cause morphologic dysplasia is long and includes infection, medications, autoimmune processes, nutritional deficiencies, and myeloid neoplasms. Follow-up of concurrent cytogenetic and molecular tests is essential for further classification; however, a normal karyotype does not fully rule out a myelodysplastic syndrome.
Copper deficiency is notorious for being a mimicker of MDS, and supplementing copper and observing the patient's CBC and possibly repeating a biopsy may be necessary in this patient. While definitely a possibility, this case is not classic for pure copper deficiency. Thrombocytopenia is less common, and the classic morphologic findings in copper deficiency are dysplasia in the erythroid lineage with cytoplasmic vacuoles in the erythroid and granulocytic lineages.
Myelodysplastic syndrome can be a difficult diagnosis to make in a patient newly presenting with cytopenias. It is rarely correct to make the diagnosis on a first biopsy, as many things must be ruled out both clinically and by using additional laboratory and molecular data. Cases such as this highlight the importance of clinical history and a close working relationship between the pathologist and clinician.