Case History
A 67 year old woman with B12 deficiency undergoes endoscopy which shows nodular gastric atrophy.
What is the presumed diagnosis?
-
A. Autoimmune atrophic gastritis
B. Zollinger Ellison syndrome
C. Environmental metaplastic atrophic gastritis
D. Sporadic neuroendocrine tumor
Answer: A. Autoimmune atrophic gastritis
Discussion:
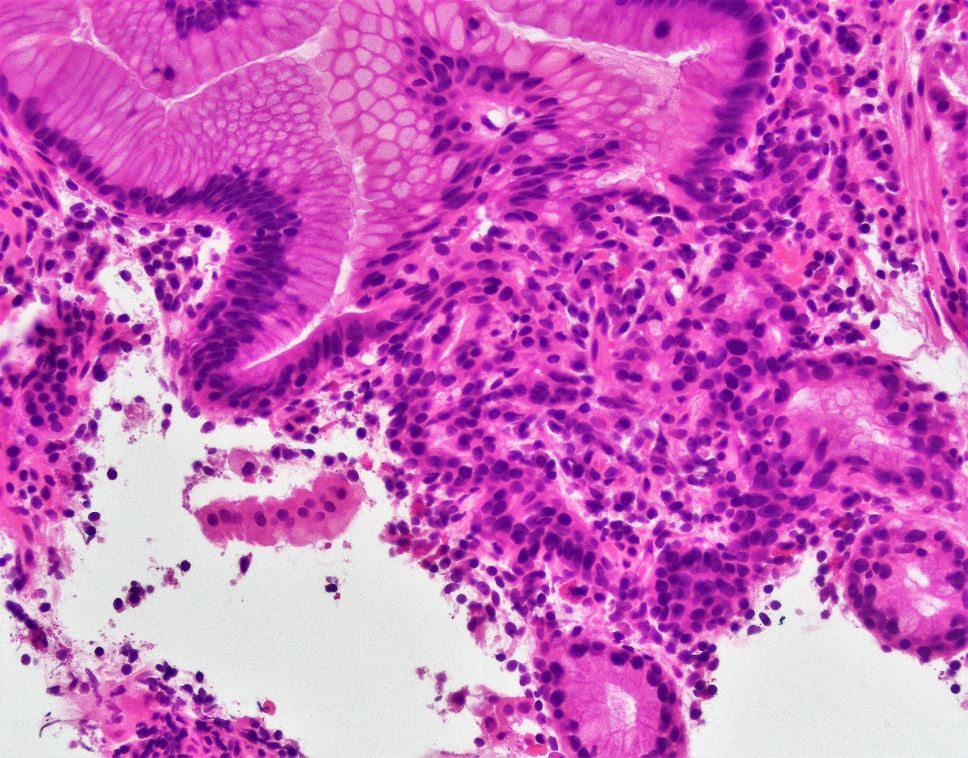
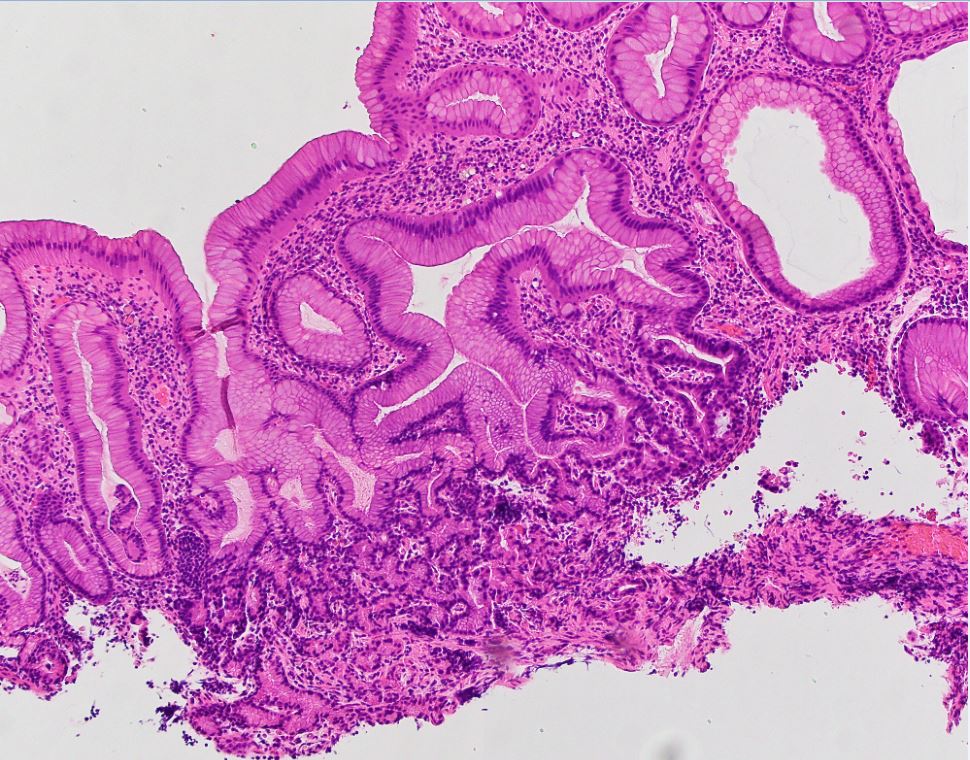
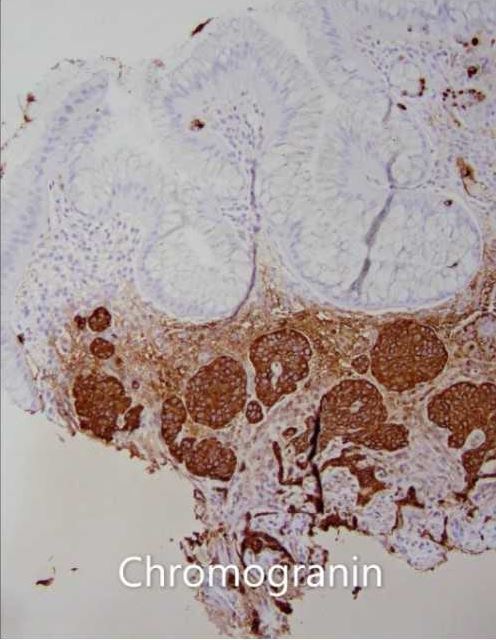
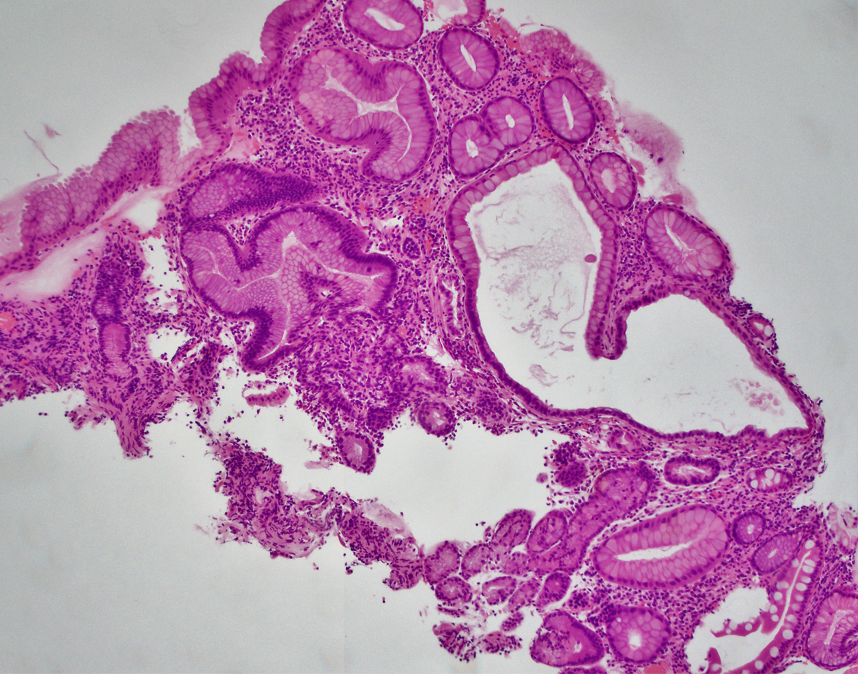
Pernicious anemia has a classically described insidious onset with nonspecific symptoms such as fatigue and headache that worsen as the disease progresses to such manifestations as cardiac symptoms, neurologic deficits, and neuropsychiatric illness. Also known as autoimmune gastritis, autoimmune atrophic gastritis, or autoimmune chronic atrophic gastritis, it is caused by inflammation due to autoantibodies to intrinsic factor and parietal cell membrane proton pumps (H+/K+ ATPase). Over time, the chronic inflammation and parietal cell destruction caused by this autoimmune reaction leads to vitamin B12 (cobalamin) deficiency and gastric atrophy with loss of oxyntic mucosa. As the oxyntic mucosa becomes more depleted, the corresponding hypochlorhydria results in an exaggerated endocrine feedback loop between the antrum and body/fundus of the stomach. Gastrin secreted by the antrum stimulates endocrine cell proliferation in the proximal stomach. The cumulative effects of the endocrine feedback loop and cell destruction induced by the chronic inflammation results in a distinct geographic atrophy of the proximal stomach. Histologically, this is characterized by chronic gastritis with oxyntic glandular dropout, foveolar hyperplasia, intestinal metaplasia, and neuroendocrine cell hyperplasia/dysplasia. Over time the neuroendocrine cell hyperplasia/dysplasia progresses to discrete neuroendocrine tumor formation (type 1 gastric neuroendocrine tumor). The differential diagnosis upon recognizing a gastric biopsy specimen exhibits chronic atrophic gastritis also includes at least Zollinger Ellison syndrome and chronic H. pylori related atrophic gastritis (environmental metaplastic atrophic gastritis/EMAG). Endoscopically, Zollinger Ellison syndrome and EMAG are classically associated with diffuse gastric atrophy as opposed to proximal gastric atrophy in autoimmune atrophic gastritis. Zollinger Ellison syndrome and autoimmune gastritis are both associated with neuroendocrine tumor formation due to hypergastrinemia. However, Zollinger Ellison syndrome associated neuroendocrine tumors (type 2 gastric neuroendocrine tumors) are present in a background of concomitant hyperchlohydria in contrast to autoimmune gastritis. All three entities are associated with increased risk of gastric adenocarcinoma.
Note: sporadic neuroendocrine tumors of the stomach are subcategorized as type 3 gastric neuroendocrine tumors
References:
Htut et al. Pernicious anemia: Pathophysiology and diagnostic difficulties. J Evid Based Med. 2021 May;14(2):161-169.doi: 10.1111/jebm.12435
Botezatu et al. Chronic atrophic gastritis: an update on diagnosis. Med Pharm Rep. 2021 Jan; 94(1): 7–14.PMID: 3362904