Case History
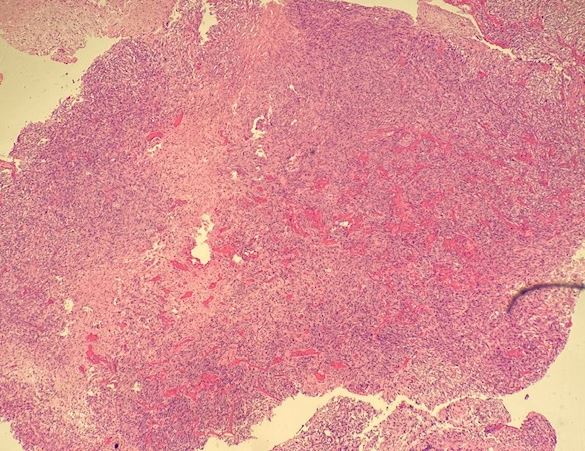
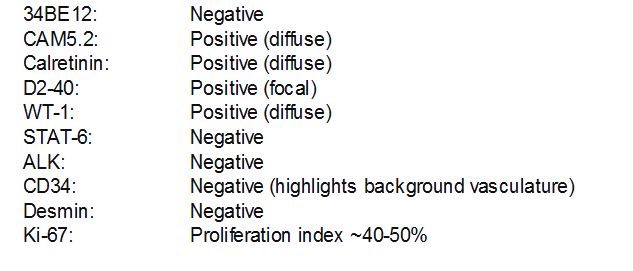
A 46-year-old female without a significant past medical history presented for symptomatic pericardial effusion with dyspnea. CT scan showed a very large primarily left-sided anterior mediastinal mass. Refer to image 4 for immunostains.
What is the diagnosis?
- Mesothelioma
- Hodgkin Lymphoma
- Thymoma
- Solitary Fibrous Tumor (SFT)
Answer: A. Mesothelioma
Explanation:
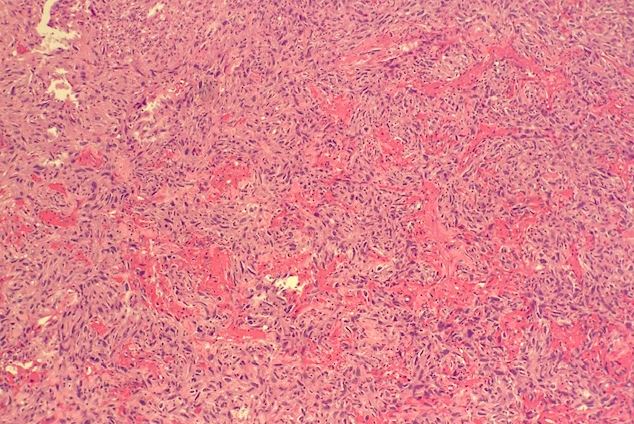
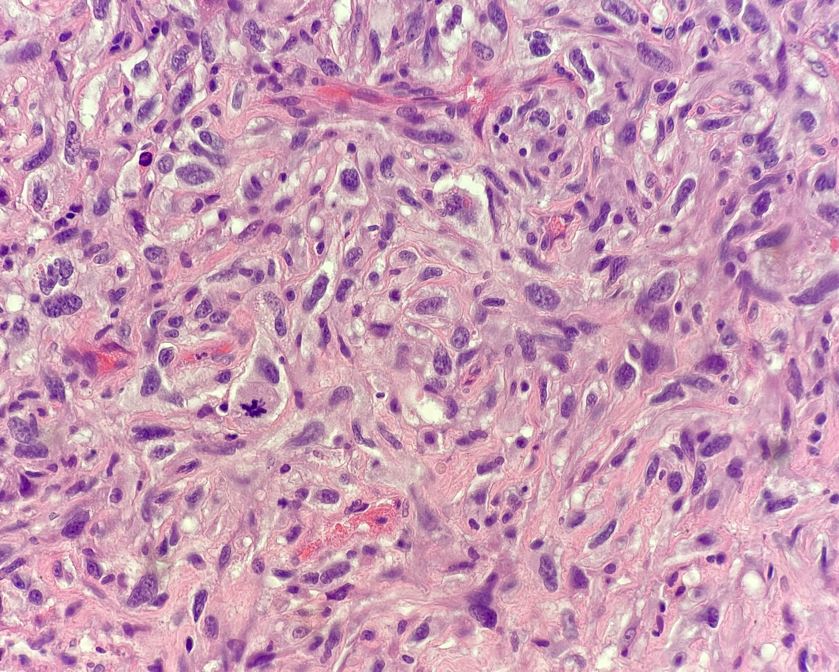
Malignant mesothelioma is an aggressive tumor of mesothelial cell origin and arises in the pleura, peritoneum or pericardium. Sarcomatoid mesothelioma is a form of malignant mesothelioma. Histologically, the appearance is that of closely packed, elongated spindle cells with an admixed chronic inflammatory infiltrate. It can also have large atypical cells, as seen in the initial photographs. Sarcomatoid mesothelioma can also occur in conjunction with another form, desmoplastic mesothelioma, which is less cellular with a storiform growth in a fibrous, sclerotic stroma. Mesothelioma, including our case, stains with mesothelial markers WT1, calretinin and D2-40. It can also stain with CK 5/6. It often has a poor prognosis with a high mortality rate and median survival rate of 7 months. Loss of nuclear BAP1 favors malignant mesothelioma over reactive/atypical mesothelial proliferation. However, this only occurs in ~ 50% of cases and is even much less common in sarcomatoid/desmoplastic malignant mesothelioma. Deletion of p16 (CDKN2A) by FISH in up to 80% of cases of pleural malignant mesothelioma and 25% of peritoneal mesothelioma can aid in diagnosis and is most commonly found in the sarcomatoid variant.