Case History:
Lung nodule FNA from a female with bilateral pulmonary nodules and a history of primary breast neoplasm.
Which of the following is most likely linked to this tumor?
A. Graded by stromal growth
B. HRAS or PIK3CA mutation
C. > 90% cribriform pattern
D. MYB/NFIB genes mutations
Correct Answer: B. HRAS or PIK3CA mutations (diagnosis is malignant adenomyoepithelioma)
Discussion:
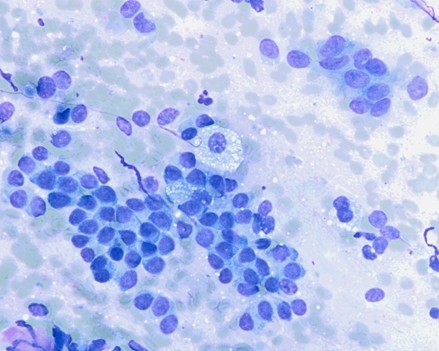
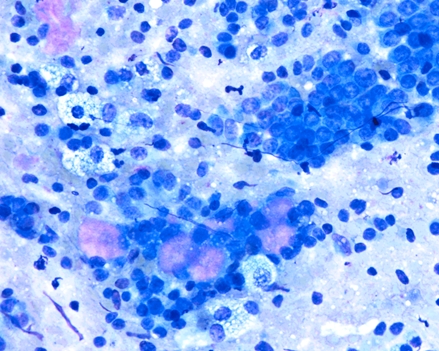
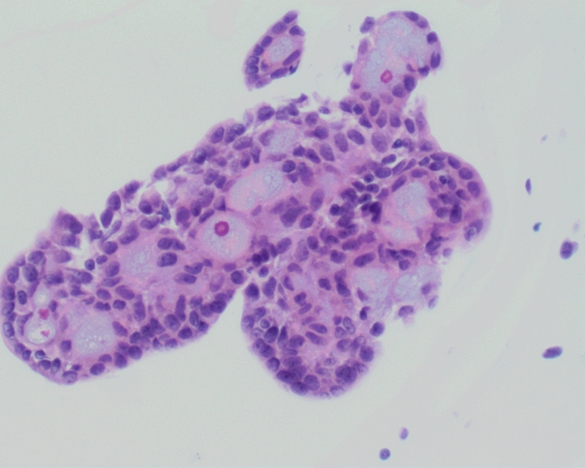
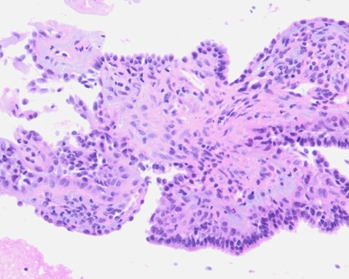
The specimen was moderately cellular and showed groups of atypical epithelial cells, along with a background of myoepithelial cells that were focally clustering and showing plasmacytoid morphology with occasional pleomorphism. The smears also showed rare cribriform and tubular-like architecture. Rare fragments of extracellular matrix material were identified. The cellblock sections highlighted vague papillary architecture with a rare cribriform morphology and some pleomorphism of the myoepithelial cells.
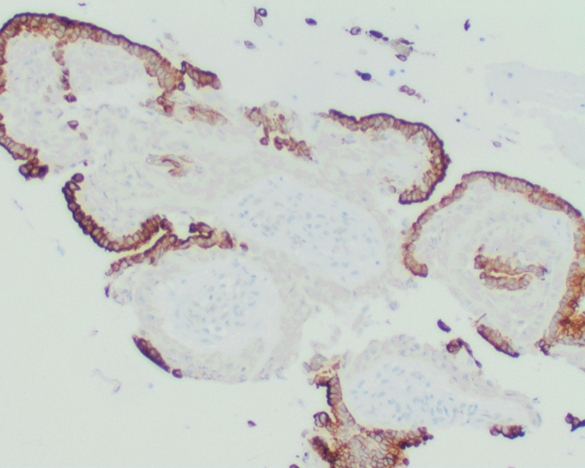
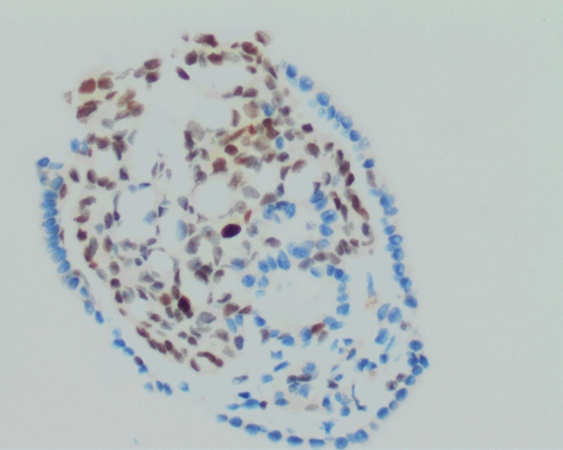
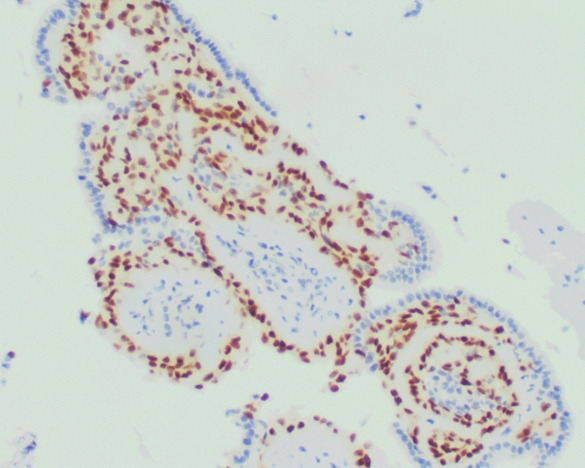
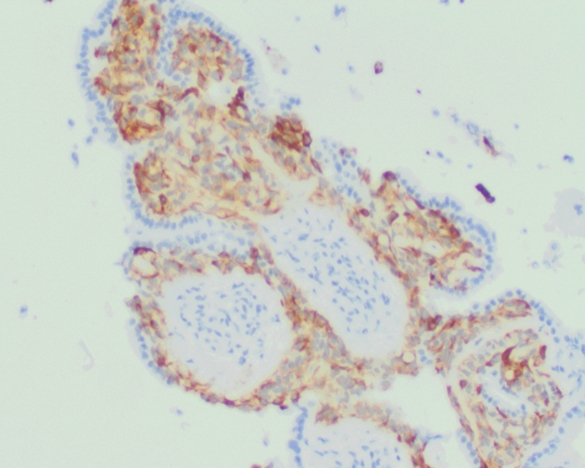
The immunohistochemical stains showed epithelial cells positivity for AE1/AE3 and focal positivity for TTF-1, with the myoepithelial cells positive for SMM, Calponin, CK5/6, and GATA-3.
In our lung FNA case, the epithelial cells were negative for GATA-3 and focally positive for TTF-1, which is most suggestive of metastatic myoepithelial component of the breast adenomyoepithelioma with likely entrapped benign respiratory epithelium.
The overall findings were compatible with the patient’s known history of breast malignant adenomyoepithelioma with lymph node metastasis.
Adenomyoepithelioma is a rare biphasic tumor with epithelial and myoepithelial components. It usually displays benign to low grade malignant behavior and a propensity for recurrence. Either epithelial or myoepithelial component can show malignant transformation. The tumor could show HRAS, PIK3CA or AKT1 mutations.
Options 1,3 and 4 are suggestive of phyllodes tumor, cribriform carcinoma and adenoid cystic carcinoma, respectively. For Phyllodes tumor and cribriform carcinoma, the morphology and staining pattern weren’t typical for these entities.
Adenoid cystic carcinoma is associated with MYB-NFIB fusion, not mutations as described in option 4. Also, the morphology showed occasional papillary architecture, rare cribriforming and abundant discohesive monomorphic plasmacytoid myoepithelial cells. Therefore, in view of the patient's history, this makes adenoid cystic carcinoma unlikely. However, ruling out adenoid cystic carcinoma by IHCs and Molecular studies is important due to the overlap in morphology between both tumors.
References:
https://www.webpathology.com/images/breast/rare-breast-tumors/adenomyoepithelioma/33963https://www.pathologyoutlines.com/topic/breastadenomyo.html
Case contributed by:
Mohamed Zedan, M.D., Cytopathology Fellow