|
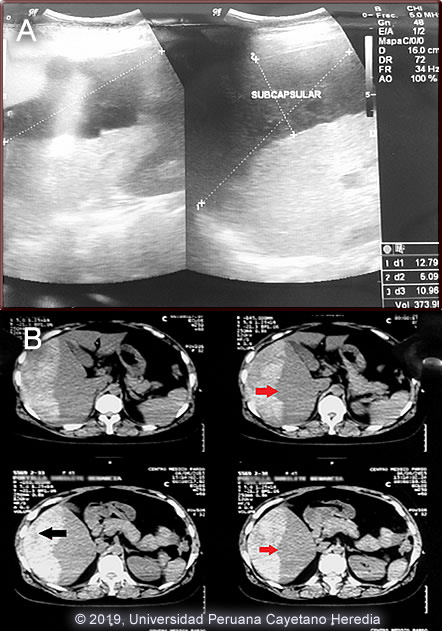
Diagnosis: Subcapsular liver hematoma due to Fasciola hepatica infection (acute phase)
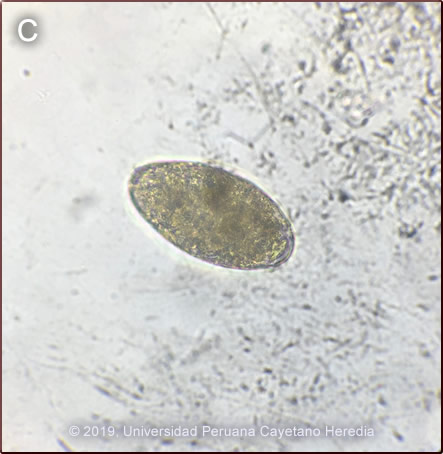
Discussion: IgG Fas2 ELISA was positive for Fasciola hepatica. Eggs of F. hepatica were observed in stool samples [Image C]. On further questioning, the patient admitted frequent consumption of lettuce and raw watercress.
Fasciola hepatica is a trematode (fluke or flatworm) in which the mature adult parasites inhabit the large biliary ducts. As with all other trematodes, Fasciola hepatica requires a snail intermediate host. Eggs produced by the hermaphroditic adults pass with the feces and hatch, releasing larvae in fresh water. After passing through a snail, mature cercariae emerge and rapidly encyst on various kinds of aquatic vegetation such as watercress. After ingestion by a human or animal definitive host, the metacercariae excyst in the duodenum and larvae penetrate the intestinal wall and subsequently directly into the liver via Glisson’s capsule embarking on a destructive migratory process through the hepatic parenchyma for 3-4 months until they reach large biliary ducts where they mature to adults. As in this case, migration through a capsular vessel may result in significant hemorrhage. The mature adults are from 1-3 cm long and attach to the biliary epithelium by a single ventral sucker. In the absence of direct visualization of adults, characteristic eggs can be seen on stool examination, but more often patients present in the early migratory phases of infection prior to maturation of the worm and the onset of egg-laying. Specific serology is the test of choice but lacks sensitivity. More modern methods including PCR amplification have shown higher sensitivity and specificity than the current standard [Am J Trop Med Hyg 2017;96(2):341].
The distribution of Fasciola hepatica is cosmopolitan, but is by far the most common in sheep-raising areas where herbivores are common definitive hosts [Curr Opin Infect Dis 2018;31(5):409]. Heavily infected sheep develop “sheep liver rot”. Other important definitive hosts are goats, cattle, horses, llamas, vicunas, and camels. The contiguous Altiplano regions of the Peruvian and Bolivian Andes are highly endemic, with human prevalence rates of as high as 67% in some villages. Egypt, Cuba, and Northern Iran are also highly endemic and the parasite is emerging in Vietnam and Cambodia. Cooking, which would kill the metacercariae, dramatically changes the flavor of watercress and the population is reluctant to adopt this simple measure.
Clinically, the disease can be divided into acute and chronic phases. During the acute phase, migrating parenchymal larvae generally cause fever, eosinophilia, right upper quadrant pain and especially significant anorexia. Vomiting and weight loss of 20 kg or more may develop, which usually abates when the larvae mature to adults. The adult flukes in the biliary tree are generally asymptomatic but some patients develop chronic manifestations including right upper quadrant pain, nausea, vomiting, and hepatomegaly. Eosinophilia and abnormal liver function may develop but are less common than with acute disease. Adult flukes may cause hyperplasia, desquamation, thickening, and dilatation of the bile ducts. We have reported a case series with clinical findings and evolution of disease [Am J Trop Med Hyg. 2008;78:222-7]. Please see Gorgas Case 2005-02 for a CT image of the typical larval tracks seen in acute disease and as well direct visualization of adult flukes via ERCP.
The differential diagnosis of eosinophilia with accompanying destructive hepatic lesions is limited. Toxocariasis causes hypereosinophilia with hepatomegaly but the pathology results from small granulomas around individual non-migrating larvae and not the large destructive lesions seen in our patient. Eosinophilia is common in Perú so it may be due to an unrelated event present concomitantly with a bacterial liver abscess; this had been the initial impression in this case.
Subcapsular liver hematoma is a rare complication of acute fascioliasis. Very few cases have been reported in the medical literature [Am J Trop Med Hyg 2019;100(3):588; Clin Infect Dis 2011;52(9):1137; Rev Gastroenterol Peru 2003;23(2):142]. While most of these cases required only medical treatment and careful clinical observation with regular hemoglobin measurements, some patients developed hemodynamic instability and required surgical intervention.
Fasciola hepatica is the only trematode infection for which praziquantel is not the drug of choice. WHO has put the anthelmintic triclabendazole (Egaten, Novartis) on its essential drugs list. Egaten is registered in Perú (as in Mexico and Egypt) and is available via free donation from the WHO. Egaten has been recently approved by the US FDA and will be available free of charge in the USA. The usual dosage is 10mg/kg with a meal. Many practitioners repeat the dosage 12-24 hours later.
Our patient was treated with a two-day regimen of 10 mg/kg/day of triclabendazole. The hemoglobin dropped to 7.8 g/dl over a period of one week of observation but no hemodynamic instability occurred. Interestingly, stool samples were positive for eggs [Image C] after 3 months of therapy and remained positive after two additional cycles of triclabendazole in absence of subsequent exposure. Failure to eliminate eggs of F. hepatica after repeated cycles of triclabendazole has been reported in Cuzco [PLoS Negl Trop Dis 2016;10(1):e0004361]. No consensus on how to treat these patients does exist, higher doses of triclabendazole for 2 days are recommended.
|